
While you may no longer need to worry about your cycles, you may still struggle with symptoms of polycystic ovarian syndrome (PCOS) in menopause. On average women enter menopause around age 51, with PCOS women experiencing menopause about two years later compared to women without PCOS.
PCOS doesn’t just go away in menopause. In fact, the metabolic and high androgen symptoms that are the hallmark of PCOS may increase—putting you at risk for several chronic conditions.
In this article, we’ll explore the relationship between PCOS and menopause, including how PCOS symptoms can change with age, management strategies, and long-term considerations of having PCOS on your heart, hormones, and overall health.
You're in ✦
Check your inbox. Day one is on its way.
Your ADHD Hormone & Brain Sync Guide is heading to your inbox now — look for it from Dr. Brighten in the next few minutes.
New Book · Out October 6, 2026
The full system behind the guide
These five days are the doorway. ADHD and Women is the whole map — the ADHD-Hormone Profile and what to do across every hormonal transition.
Pre-Order ADHD and WomenIn this article
The Hormone Connection Between PCOS and Menopause
PCOS is a hormonal and metabolic disorder that is characterized by irregular menstrual cycles, elevated testosterone levels, and in some cases, ovarian cysts.
A common symptom of PCOS is irregular menstrual periods or missing periods due to disrupted ovulation. This condition can also make it hard for women to get pregnant.
Women with PCOS have lower levels of progesterone due to irregular ovulation or anovulation (when you don’t ovulate). When ovulation becomes more irregular in perimenopause (the transition period into menopause) and stops with menopause, progesterone levels will also be low.
In many causes, insulin dysregulation is present, leading to increased production of testosterone from the ovaries, weight gain, and risk of type 2 diabetes.
The exact cause of PCOS isn’t known, but it often runs in families—meaning there is a genetic component.
Symptoms of PCOS include:
- Irregular periods
- Excessive hair growth where you don’t want it (hirsutism)
- Hair loss where you do want it (on your scalp)
- Acne
- Trouble losing weight
- Anxiety
- Depression
Menopause, on the other hand, is not a disorder but a natural phase in women’s lives. Menopause marks the end of reproductive years, typically occurring around the age of 51, when menstrual periods cease due to declining ovarian function.
Prior to menopause, perimenopause hormones begin with a decline in progesterone, leaving some women in a hyperestrogen state (what some people refer to as estrogen dominance). This state of unchallenged estrogen (meaning there is not adequate progesterone to counter the effects of estrogen) can also occur in anovulatory cycles of PCOS
Perimenopause can last up to 10 years and commonly causes symptoms like:
- Irregular menstrual cycles
- Hot flashes
- Sleep disturbances
- Mood swings
- Weight gain
- Changes in skin, including acne
- Hair loss
- And many other symptoms, which you can read about here
Perimenopause is the transition period before menopause, during which a woman’s body eventually makes less and less estrogen until estrogen production stops altogether in menopause.
How Hormones Vary in PCOS, Perimenopause and Menopause
| Hormone | PCOS | Perimenopause | Menopause |
| Estrogen | High or Normal | Fluctuates | Low |
| Progesterone | Low | Low | Low |
| Testosterone | High | Normal | Varies between individuals |
Testosterone Levels in Menopause
High testosterone symptoms like hirsutism (unwanted hair growth), oily skin, acne, and female pattern baldness are common in PCOS. Unfortunately, in menopause some of these symptoms may persist.
As many as 50% of women report hair loss in menopause, with PCOS women potentially experiencing more devastating effects due to the years of high androgen exposure to their hair.
While the ovaries will discontinue androgen production, the adrenal glands supply roughly 50% of a woman’s testosterone.
In cases of adrenal PCOS, DHEA is produced and converted into testosterone, leading to high androgen symptoms.
This doesn’t mean a woman with PCOS will not be a candidate for testosterone hormone replacement therapy or won’t experience symptoms of low testosterone. Rather, testing of free and total testosterone, along with a symptom intake, should be done to determine if this treatment is best.
Can PCOS Cause Early Menopause?
PCOS has been shown to affect the age1 at which women naturally experience menopause. Women with PCOS often experience later menopause, sometimes by 2-5 years.
In addition, there have been multiple studies2 showing that women with PCOS may have more successful fertility outcomes later in life due to a slower decline in age related fertility. Women with PCOS should be aware that:
- They may still be able to become pregnant during perimenopause.
- They should meet with a reproductive endocrinologist to discuss their personal fertility goals sooner than later in order to have the best outcomes.
Menopause and Polycystic Ovarian Syndrome Risk Factors
Studies show3 that with increased age and loss of estrogen, the metabolic risk factors of PCOS increase—affecting the heart, immune system, brain, and more.
On its own, PCOS increase the risk of:
- Insulin resistance and type 2 diabetes
- Stroke
- Heart attack
- High cholesterol
- Weight gain, weight loss resistance, obesity
- Chronic inflammation
When women transition into menopause, there is an increased risk of:
- Insulin resistance and type 2 diabetes
- Stroke
- Heart attack
- High blood pressure
- Metabolic syndrome
- Weight gain, specifically increased visceral adiposity (belly fat)
- High cholesterol, specifically elevated LDL and triglyceride levels
PCOS or Perimenopause Symptoms

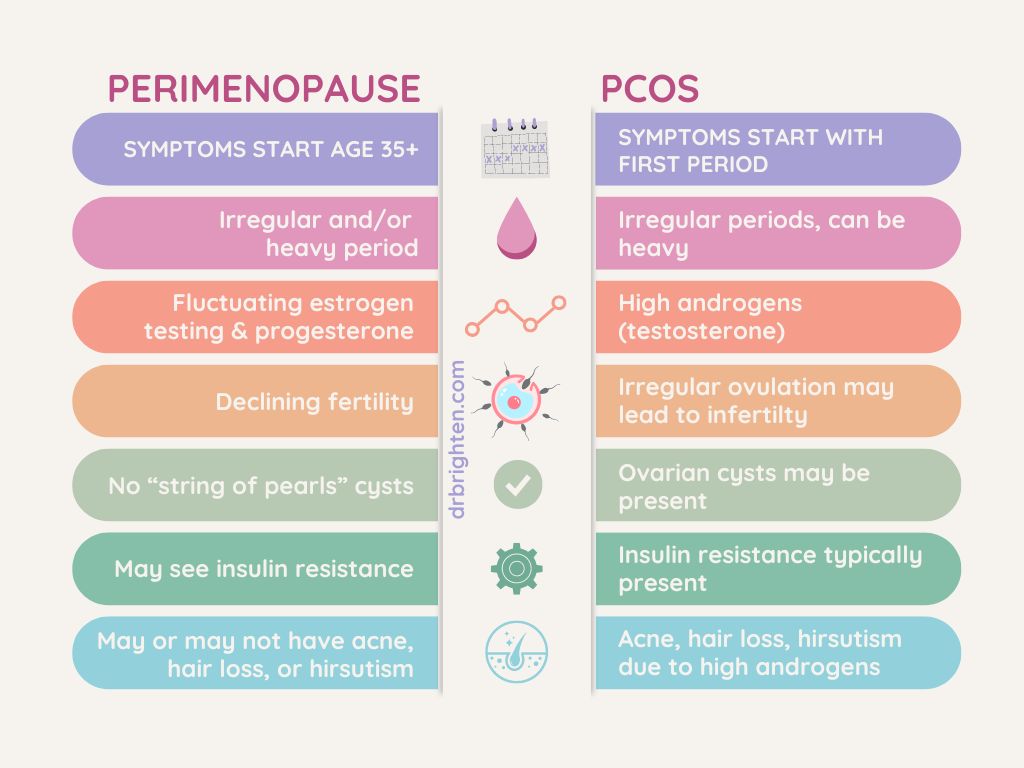
Some symptoms of PCOS, perimenopause, and menopause might seem to overlap, but they’re underlying causes are different, and they’re treated in unique ways.
Perimenopause and PCOS can mimic each other due to fertility issues and irregular periods, although some symptoms occur in perimenopause that don’t affect most women with PCOS.
Here’s how the symptoms of these conditions compare:
| Symptom | Perimenopause | PCOS |
| Irregular Periods | Common | Common |
| Menstrual Cycle Changes | Yes, often shorter or longer cycles | Yes, typically irregular or absent periods |
| Hormonal Fluctuations | Yes, fluctuating estrogen and progesterone levels | Yes, high androgen levels. May also have high estrogen. |
| Hot Flashes | Yes, common | No |
| Ovarian Cysts | No | Yes, common |
| Fertility Concerns | Decreased fertility | Difficulty conceiving due to irregular ovulation |
| Decreased Libido | Common | May be present, but not a common symptom |
| Hair Loss | Yes, general thinning | Yes, often in the temporal area |
| Hirsutism (thick, coarse hair on face) | Yes, may be present, especially the closer one is to menopause | Yes, often present |
| Weight Gain | Yes, common | Common, but not present in every PCOS case |
| Urinary Incontinence | Yes, late perimenopause and menopause with decline of estrogen | No |
| Urinary Tract Infections (UTIs) | Yes, common with decline of estrogen | No |
| Sleep Disturbance | Yes | Yes |
Is It PCOS or Perimenopause?
If you’re in your 40s or early 50s and have had a diagnosis of PCOS in the past, you might be seeking help in differentiating between perimenopause and PCOS. The difference lies in hormonal profiles, menstrual patterns, and clinical symptoms:
One of the greatest differentiating factors is when the symptoms began. PCOS is a lifelong condition, with signs of ovulatory dysfunction at a very young age.
Perimenopause, on the other hand, will not present until mid-life or within the 10 year window of anticipated menopause.
Does PCOS Go Away After Menopause?

PCOS is primarily driven by hormonal imbalances involving insulin resistance and androgen excess, which are the causes of ovarian dysfunction and menstrual irregularity. There is also evidence of a gut component that may contribute to PCOS developing.
While the irregular periods associated with PCOS typically resolve after menopause (which is the cessation of menstruation), the metabolic and cardiovascular risks can persist4 or even worsen.
Women with PCOS are at increased risk5 of developing obesity, type 2 diabetes, and cardiovascular disease later in life. That’s because these conditions are influenced by lifelong hormonal and metabolic dysregulations6 as well as chronic inflammation.
So, while irregular periods might not be an issue anymore during the menopausal years, this doesn’t mean that hormonal health isn’t important or something to be concerned about.
Additionally, for women with PCOS, the menopause transition can exacerbate PCOS symptoms such as insulin resistance, weight gain, and cardiovascular risks. During perimenopause and menopause, declining estrogen levels lead to changes in hormone production and metabolic function that can worsen PCOS symptoms.
Some women with PCOS might find that they need to work even harder to manage symptoms while entering perimenopause, such as by taking really good care of themselves with a healthy diet, exercise, sleep, and stress management. All of these steps are important in the long term for decreasing the risk of health complications such as heart disease.
Tips for Managing PCOS Through Menopause
Given the ongoing risks that hormonal issues can cause, it’s essential for women with PCOS to continue health monitoring and maintain a healthy lifestyle even after menopause.
To help navigate and manage PCOS during menopause, you want to work on addressing underlying hormonal imbalances, metabolic health, and long-term risk factors for issues like cardiovascular disease.
| Evidence Based Strategies for PCOS Through The Menopause Transition | How to Implement |
| Low glycemic, high fiber, whole foods nutrition. | Go by the 80/20 rule and aime to have 80% of your foods be nutrient dense. Include adequate protein in your meals, here’s how. Use the recipe guide here to help you get started. |
| Exercise | 150 minutes total per week Use this list of exercise ideas to get started. |
| Myoinositol | Myoinositol 2,000 mg/ day to support healthy blood sugar, ovarian function, and sleep Myoinositol Plus |
| Estrogen and progesterone supporting herbs and nutrients | Vitex, selenium, vitamin B6, C, Calcium d-glucarate Balance Women’s Hormone Support |
| Adaptogenic herbs | Rhodiola, Holy Basil, Ashwagandha, Eleutherococcus, Shatavari (asparagus racemosus). These help support adrenal function, a source of hormones in menopause and a common cause of hormone imbalance in PCOS. Adrenal Support – morning formula Adrenal Calm – evening formula |
| Probiotics | Lactobacillus, Bacillus, S. boulardiii, Bifido species Women’s Probiotic with Prebiotic |
| Magnesium | Magnesium glycinate 300 mg/ day to support healthy bones, brain, mood, and sleep Magnesium Plus |
| Androgen Balancing Herbs | Saw Palmetto, Spearmint, Nettle Root. These can help with hirsutism and hair loss. Saw Palmetto Plus Myoinositol Plus |
| Sleep Supportive Herbs and Nutrients | Passion flower, Ashwagandha, PhosphatidylSerine, L-Theanine. These promote restorative sleep and circadian rhythm health. Adrenal Calm |
| Omega 3 Fatty Acids | Balances inflammation, supports brain health, assists in insulin and blood sugar optimization Omega Plus |
| Hormone Replacement Therapy (HRT) | Oral micronized progesterone nightly Topical estradiol in late stage perimenopause and menopause These should always be under a doctor’s supervision. |
| Androgen Blocking Medication | Spironolactone and other medications can be used to prevent hirsutism and hair loss. These should only be used under a doctor’s supervision. |
The strategies below can be very helpful for supporting metabolic health during and after menopause:
Lifestyle Modifications:
- Diet: Eat a low-glycemic index diet rich in fiber, protein, and healthy fats from whole grains, fruits, vegetables, nuts, seeds, olive oil, and lean proteins to manage insulin levels and lose weight more easily if necessary.
- Exercise: Regular physical activity improves insulin sensitivity, aids in weight management, and reduces inflammation and cardiovascular risks.
- Intermittent fasting: Fasting during menopause, and if you have PCOS, is a tool that can assist in weight loss, improve insulin sensitivity, and provide benefits for lowering inflammation and supporting heart health.
Supplements:
A number of menopausal supplements can help with balancing hormones and improving quality of life, such as:
- Phytoestrogens and isoflavones that mimic natural estrogen’s effects7
- Antioxidants, including resveratrol that reduce oxidative stress
- Adaptogens and herbs such as ashwagandha, black cohosh, and vitex (chaste tree berry) support overall hormonal balance
- Vitamin D which assists in hormone production and inflammation management
- Magnesium and calcium that support hormone metabolism and bone and heart health
- Probiotics that assist in healthy gut function
- Myoinositol to support blood sugar and insulin, along with ovarian function and sleep
- Omega-3 Fatty Acids that support cellular health, balances inflammation, and helps with blood sugar optimization
I’ve written extensively on many supplements that can support hormones during different stages of life, so you may want to read these articles for more information and guidance:
- Best Menopausal Supplements
- 15 Perimenopause Supplements for Happy Hormones
- The Best Herbs for Menopause
- Supplements for PCOS
Hormonal Therapy:
- Hormone Replacement Therapy (HRT): Discuss HRT with your healthcare providers for personalized hormone therapy options. These medications are prescribed to alleviate menopausal symptoms like hot flashes and vaginal dryness.
- Anti-androgen medications: Discuss the use of anti-androgens with your provider or help in managing persistent androgen-related symptoms post-menopause, such as hirsutism and acne.
Regular Monitoring, Screening, and Support:
- Cardiovascular health check-ups: Monitor your blood pressure and cholesterol levels and undertake cardiovascular risk assessments regularly.
- Diabetes screenings: Due to the increased risk of insulin resistance and type 2 diabetes, routine glucose monitoring and HbA1c tests are recommended.
Long-term Health Risks for PCOS Patients After Menopause
If you have PCOS in your reproductive years, you’re at greater risk for health issues8 as you age, including:
- Cardiovascular disease: PCOS is associated with an increased risk of heart disease, which persists after menopause.
- Type 2 diabetes: Insulin resistance, common in PCOS, continues to be a risk factor for diabetes post-menopause.
- Metabolic syndrome: The cluster of conditions, including high blood pressure, high blood sugar, and abnormal cholesterol levels, remains a concern as someone ages past their 50s.
- Endometrial cancer: The risk may decrease after menopause, but it’s still higher than in women without PCOS history.
- Obesity: Weight management issues often continue, contributing to other health risks.
- Osteoporosis: While PCOS may offer some protection against bone loss, the overall risk increases after menopause.
- Sleep apnea: This condition, more common in PCOS, can persist beyond reproductive years.
These long-term risks persist because of:
- Hormonal imbalances that persist: Even after menopause, hormonal irregularities can continue to affect a woman’s metabolism9 and overall health. For example, lower estrogen levels can contribute to changes in cholesterol levels and metabolism, increasing the risk of cardiovascular disease.
- Insulin resistance: This core feature of PCOS doesn’t necessarily resolve with menopause and may get worse.
- Chronic inflammation: PCOS is associated with low-grade inflammation, which can contribute to various health issues over time. Inflammation can continue or worsen with age from factors like a poor diet, obesity, or drug or alcohol use. Additionally, autoimmune conditions can arise during menopause, giving way to more inflammation.
- Lifestyle factors: Habits and health conditions developed during reproductive years (like being overweight10, obesity, sleep deprivation, or high blood pressure) can continue to impact health post-menopause.
- Genetic factors: The genetic predispositions that contribute to PCOS remain present throughout life.
Key Takeaways on PCOS and Menopause
- PCOS and menopause represent a unique situation requiring individualized support to minimize risk factors.
- During perimenopause, changes in hormones can cause symptoms that mimic PCOS, such as irregular periods.
- Menopause can put an end to irregular periods, but still, if you had PCOS in your reproductive years, you’re at greater risk for long-term health issues tied to inflammation and hormonal imbalances, including heart disease.
- Women with a history of PCOS should remain vigilant about their health post-menopause by eating a healthy diet, exercising, managing stress, and monitoring their health markers and weight.
- For personalized guidance on managing PCOS through menopause, consult with a healthcare provider experienced in hormonal disorders and menopausal health.
References
- https://journals.lww.com/menopausejournal/abstract/2024/02000/a_prospective_study_on_the_relationship_between.8.aspx ↩︎
- https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2019.00834/full ↩︎
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8189332/ ↩︎
- https://journals.lww.com/clinicalobgyn/abstract/2021/03000/polycystic_ovary_syndrome__menopause_and.16.aspx ↩︎
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8189332/ ↩︎
- https://onlinelibrary.wiley.com/doi/10.1111/cen.14558 ↩︎
- https://pubmed.ncbi.nlm.nih.gov/31689947/ ↩︎
- https://pubmed.ncbi.nlm.nih.gov/32747035/ ↩︎
- https://pubmed.ncbi.nlm.nih.gov/37353908/ ↩︎
- https://pubmed.ncbi.nlm.nih.gov/37353908/ ↩︎