


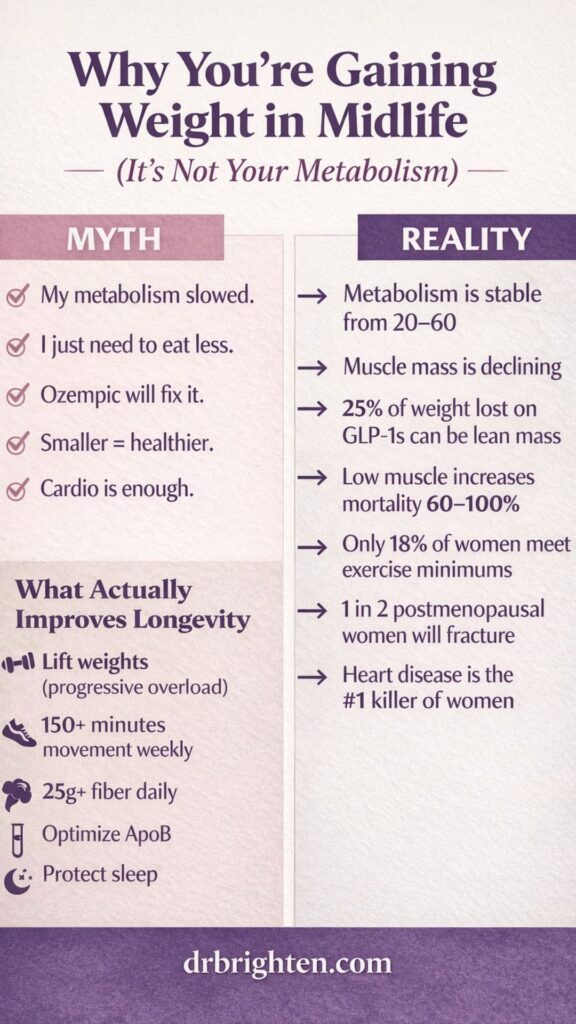
Midlife weight gain is often blamed on a “slowing metabolism.” But the science tells a different story.
Between ages 20 and 60, your metabolism barely changes. What does change? Muscle mass. Exercise habits. Hormonal signaling. Cardiovascular risk. And increasingly, the conversation around GLP-1 medications like Ozempic.
In this episode, we unpack the real drivers of midlife weight gain, the surprising data on muscle loss and mortality, the nuanced role of GLP-1 drugs in long-term health, and what actually improves lifespan and healthspan.
If you’ve wondered:
- Is my metabolism broken?
- Is Ozempic helping or hurting long term?
- Why is muscle suddenly such a big deal?
- What actually prevents heart disease and dementia?
This episode connects the dots.
What You’ll Learn About Midlife Weight Gain, Ozempic, and Muscle Loss
In this conversation, we go beyond surface-level advice and into evidence-backed physiology. Here’s what you’ll discover:
- Why your metabolism does NOT meaningfully slow between ages 20 and 60
- The real reason most women gain weight in their 40s and 50s
- Why only 18% of women in their 50s–60s meet minimum exercise guidelines
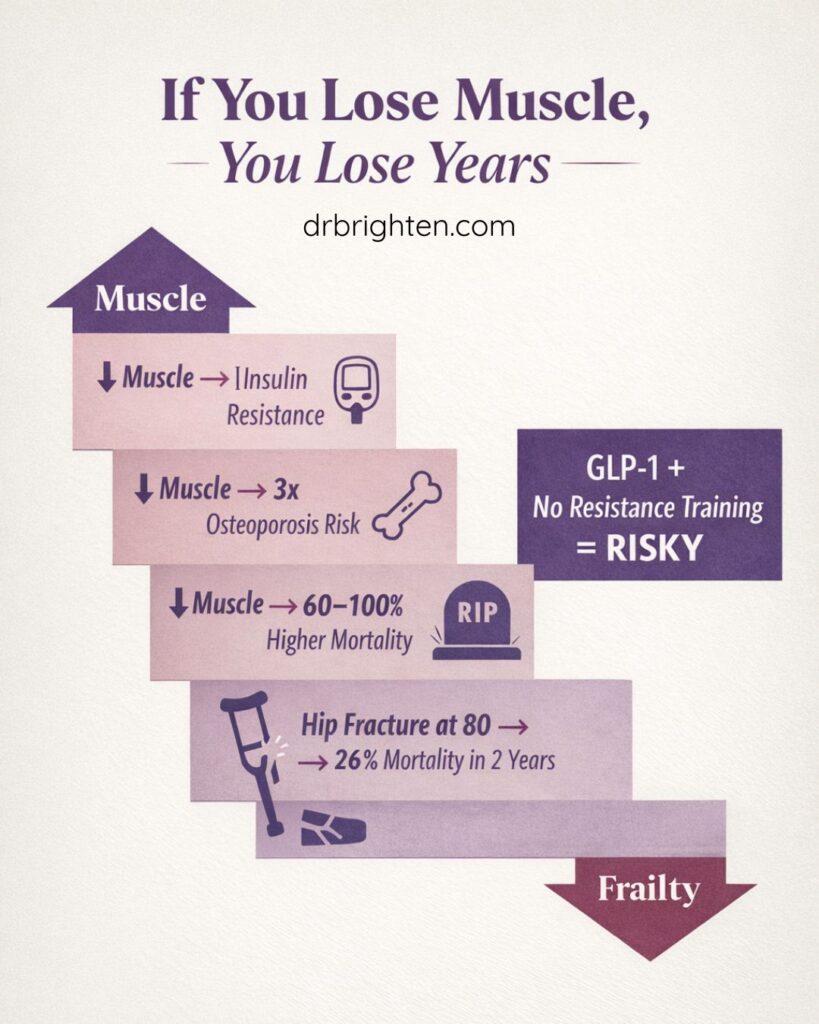
- How losing muscle increases mortality risk by 60–100%
- Why shrinking your body does not automatically mean better health
- The truth about GLP-1 medications like Ozempic and lean mass loss (about 25% of weight lost)
- Why muscle loss dramatically increases osteoporosis risk (3x higher)
- The sobering statistic: 1 in 2 postmenopausal women will have an osteoporotic fracture
- What happens after a hip fracture: up to 1 in 4 women over 80 die within two years
- Why heart disease—not breast cancer—is the #1 killer of women
- How lowering ApoB can reduce heart disease risk by 85%+
- The difference between acute inflammation (like after exercise) and chronic systemic inflammation
- Why fiber may be one of the most underrated tools in metabolic health
- The top four modifiable dementia risk factors accounting for 30% of global cases
- Why progressive overload in strength training matters more than random workouts
- Why smaller ≠ healthier when muscle is sacrificed
Each point builds toward a central idea: weight in midlife is not just about fat — it’s about muscle, metabolic resilience, and long-term survival.
Does Metabolism Actually Slow in Midlife?
This is one of the most persistent myths in women’s health.
Research shows that resting metabolic rate remains remarkably stable from age 20 to 60. After 60, metabolism declines modestly — about 0.7% per year. That’s not the dramatic collapse many people assume is happening at 45.
So what changes?
1. Movement Declines
Exercise rates drop every decade after the teenage years. Women exercise less than men at every stage of life.
By age 50–60, only 18% of women meet the American Heart Association’s minimum recommendations:
- 150 minutes of aerobic activity weekly
- 2 days of resistance training
That’s a low bar — and most women aren’t meeting it.
2. Muscle Mass Declines
Muscle is not cosmetic tissue. It’s metabolically active.
Muscle:
- Improves insulin sensitivity
- Increases basal metabolic rate
- Releases anti-inflammatory myokines
- Supports nitric oxide production for vascular health
- Facilitates insulin-independent glucose uptake
Low muscle mass (sarcopenia) increases mortality risk by 60–100%.
3. Hormones Shift
Estrogen decline changes fat distribution, increasing visceral adiposity. Visceral fat is metabolically active and associated with increased cardiometabolic risk.
Hormone replacement therapy may improve fat distribution, but it does not fully normalize cardiovascular risk markers.
If you’ve been told your metabolism is broken or that weight loss alone equals health, this episode will challenge everything you thought you knew.
Listen now to understand what actually drives midlife weight gain and what protects your longevity.
Ozempic, GLP-1 Medications, and Muscle Loss: What the Data Shows
GLP-1 medications like Ozempic are changing obesity medicine.
In individuals with obesity or diabetes, these medications:
- Improve glycemic control
- Reduce cardiovascular events
- Support significant weight loss
- Reduce appetite signaling
For many patients, they are life-changing.
But here’s the nuance.
About 25% of weight lost on GLP-1 medications comes from lean mass, including muscle. Importantly, this percentage is similar to lifestyle-based weight loss.
The difference?
If someone begins at a normal weight and loses lean mass without medical indication, the risk-benefit equation shifts.
Muscle loss:
- Increases osteoporosis risk
- Increases frailty
- Raises mortality risk
- Reduces metabolic resilience
Smaller is not synonymous with healthier.
For individuals with obesity, GLP-1s combined with resistance training can improve metabolic outcomes dramatically. But using them purely as longevity “hacks” without metabolic disease requires careful consideration.
Muscle: The Real Longevity Currency
If there is one theme in this episode, it’s this:
We are over-obsessed with supplements and under-invested in muscle.
Muscle affects:
- Insulin sensitivity
- Cardiovascular health
- Inflammatory signaling
- Nitric oxide production
- Glucose disposal
- Bone density
- Functional independence
Low muscle mass triples osteoporosis risk.
One in two postmenopausal women will experience an osteoporotic fracture.
After age 80, if a woman breaks her hip, 26% will die within two years.
That statistic alone reframes the conversation around “weight loss.”
Longevity is not about being smaller.
It’s about being stronger.
Cardiovascular Risk in Midlife Women
Heart disease is the number one killer of women.
Atherosclerotic cardiovascular disease (ASCVD) is driven by elevated ApoB-containing particles (like LDL).
Lowering ApoB to optimal ranges (~50–60 mg/dL) can reduce cardiovascular risk by 85% or more.
Lifestyle matters:
- Mediterranean diet
- Exercise
- Blood pressure control
- Avoiding smoking
- Sleep optimization
But genetics heavily influence LDL and ApoB. For some individuals, lifestyle alone is not enough.
Midlife is when risk begins to rise — especially as estrogen declines.
Hormones alone are not sufficient protection.
Inflammation: What Social Media Gets Wrong
Inflammation has become a catch-all buzzword.
CRP (C-reactive protein) measures systemic inflammation. But:
- Intense exercise can temporarily raise CRP.
- That acute increase is not harmful.
- Long-term exercise reduces systemic inflammation.
Ultra-processed foods are associated with worse metabolic outcomes. However, replacing saturated fats with unsaturated fats (including certain seed oils) lowers cardiovascular risk in human trials.
Mechanistic theory does not always equal real-world outcomes.
Chronic inflammation is dangerous.
Physiologic stress responses (like exercise) are adaptive.
Heart disease is still the #1 killer of women and most women are never told their real risk. Tune in to learn what to test, what to optimize, and how to dramatically lower your lifetime risk.
Why Fiber Is the Quiet Metabolic Powerhouse
Most adults consume 7–10 grams of fiber per day.
Recommended:
- Women: at least 25 grams daily
- Men: about 35 grams daily
Fiber:
- Reduces cancer risk
- Improves satiety
- Improves insulin sensitivity
- Supports microbiome diversity
- Helps regulate appetite
Increasing fiber gradually (start low, go slow) prevents GI discomfort.
Fiber may not be trendy — but it’s foundational.
Sleep and Its Role in Weight and Longevity
Sleep affects:
- Insulin sensitivity
- Appetite hormones
- Inflammation
- Cardiovascular risk
- Dementia risk
Seven hours minimum is recommended.
Cognitive Behavioral Therapy for Insomnia (CBT-I) is one of the most effective evidence-based interventions for chronic sleep disturbance.
Start with a consistent wake time.
Build sleep pressure.
Reduce bedtime anxiety.
Sleep is not optional for longevity.
Dementia Prevention and Midlife Risk
Four modifiable risk factors account for 30% of global dementia cases:
- Sedentary lifestyle
- Untreated hearing loss
- Hypertension
- Limited cognitive engagement
Elevated LDL in midlife triples dementia risk.
Exercise, cardiovascular optimization, and ongoing learning matter profoundly.
Longevity is brain health — not just body weight.
This Episode Is Brought to You By
Dr. Brighten Essentials
Want science-backed supplements formulated by a doctor who actually understands women’s health? 🌿 At Dr. Brighten Essentials, every product is crafted to support your hormones, boost your energy, and help you feel your best—inside and out. From targeted nutrients for glowing skin to essentials that fuel your daily vitality, you’ll get the highest-quality ingredients in forms your body can truly use.
Exclusive for podcast listeners: Use code POD15 at checkout for 15% off your order.
Sunlighten Saunas —Want a gentle, science-forward way to sweat, recover, and unwind? At Sunlighten, infrared saunas deliver soothing heat that supports relaxation, muscle recovery, and deep, comfortable sweating—without the stifling temps of traditional saunas. With low-EMF tech and options for near, mid, and far infrared, you get a calm, restorative session tailored to your goals.
Exclusive for podcast listeners: use the code DRBRIGHTEN to save up to $1,400 on your sauna
LMNT Electrolytes —Want a clean, science-backed way to stay hydrated and energized? At LMNT, electrolytes are formulated with a precise balance of sodium, potassium, and magnesium — with no sugar, no artificial ingredients, and no unnecessary fillers. Designed to support hydration, muscle function, and daily energy, LMNT helps you feel your best through workouts, busy days, and everyday life.
Exclusive for podcast listeners: Visit DrinkLMNT.com/Brighten to receive a free sample pack with any purchase.
Links Mentioned in This Episode
Dr. Mary Pardee is a Naturopathic Medical Doctor specializing in preventative medicine and longevity in Los Angeles, California. She worked in exercise physiology research with the US government after college.
Mary Pardee’s Instagram: @dr.marypardee
Mary Pardee’s Website: modrnmed.com
Mary Pardee’s Youtube: @dr.marypardee7668
Related Articles:
How Much Protein Should Women Have
Breakfast with 30 grams of Protein for Hormone Balance
Tips to Help With Menopause Weight Loss
Inositol for Weight Loss and Enhancing Metabolic Health
Why Hormonal Imbalance Can Make Weight Loss Difficult
Ozempic for Weight Loss: Side Effects, Benefits, Risks
How to Lose Weight During Perimenopause
Related Episodes:
The Truth About Insulin Resistance Treatment, Foods, and Labs in Perimenopause
Why Strength Training for Women Is Not Optional for Longevity | Gabrielle Lyon
This Weight Loss Diet Helped Her Lose 100 Pounds (Without Cutting Pizza!) | Ilana Muhlstein
GLP-1 Weight Loss in Menopause: How HRT Amplifies Results
The New Perimenopause Weight Loss Approach | Tara LaFerrara
Frequently Asked Questions
Metabolism remains stable between ages 20–60. Weight gain is more commonly driven by reduced muscle mass, decreased activity, hormonal shifts, and dietary changes.
Yes. Approximately 25% of weight lost on GLP-1 medications comes from lean mass, including muscle. Resistance training is essential to preserve muscle during weight loss.
Yes. Low muscle mass increases mortality risk by 60–100% and triples osteoporosis risk.
The long-term risk-benefit ratio is unclear. Muscle preservation must be considered carefully.
Strength training and muscle preservation are significantly more impactful for long-term survival than most supplements.
Minimum: 150 minutes aerobic activity weekly + 2 days resistance training.
Greater benefits are seen with higher volumes.
Chronic inflammation can contribute to metabolic dysfunction, but acute inflammatory responses (like from exercise) are beneficial adaptations.
Transcript
Dr. Brighten: [00:00:00] Millions of people are swallowing handfuls of supplements every single day, thinking that is the hack to longevity and wellness. Is there any truth to that?
Mary Pardee: No, and I view supplements as the last little bit in longevity, not the majority of the pie. Muscle is one of the cornerstones for longevity and health span.
And so we look at sarcopenia. People with low muscle mass, they have 60 to a hundred percent higher risk of mortality, and your risk for osteoporosis triples.
Dr. Brighten: What's your take on why people gain weight as they age?
Mary Pardee: When women come in in their forties, fifties, or men and they say, oh, I'm just getting older.
My metabolism slows. I go, I'm sorry. It's not because of that.
Dr. Brighten: What if the way you're aging is optional and you could start slowing it down today,
Narrator: Dr. Mary Parti is one of the leading experts in longevity and preventive medicine,
Mary Pardee: a former performance researcher for the US government.
Narrator: She's here to break down the science of extending your years.
Strengthening your body and upgrading the quality of your years.
Mary Pardee: What do you [00:01:00] say
Dr. Brighten: if someone's worried about dementia?
Mary Pardee: Top four risk factors for dementia, that accounts for 30% of global dementia cases is gonna be number one, a sedentary lifestyle. So exercise, hearing loss, high blood pressure. And then
Dr. Brighten: what's one thing about longevity that you wish people would stop obsessing over?
Mary Pardee: There's so many things.
Dr. Brighten: Welcome to the Dr. Brighton Show, where we burn the BS in women's health to the ground. I'm your host, Dr. Jolene Brighton, and if you've ever been dismissed, told your symptoms are normal or just in your head or been told just to deal with it. This show is for you. And if while listening to this, you decide you like this kind of content, I invite you to head over to dr brighton.com, where you'll find free guides, twice weekly podcast releases, and a ton of resources to support you on your journey.
Let's dive in. This is the way to longevity and wellness. Is there any truth to that?
Mary Pardee: No, and I think this is a, a piece that people are really [00:02:00] missing the boat on, where people come in, they're on 10, 20, 30 supplements, hoping that it's going to help them live longer or improve their quality of life. And I really view supplements as the last little bit in longevity and not the majority of the pie.
Dr. Brighten: Except that all of the leaders that you see online, not set, not necessarily in the lab, in longevity, are saying, this is the new supplement. This is the thing that's gonna extend our life.
Mary Pardee: The clickbait is real. I agree with that. It's all over social media. People wanna sell things. People wanna make money, and people buy supplements.
The global nutraceutical industry itself is gigantic. We're talking trillions of dollars, and so it's an easy way to make money, and I don't think a lot of it is warranted. And so there's some interesting things that are coming out to keep your eye on, but right now in terms of should you take a supplement or should you do all of these other things that we know, 100% will extend your [00:03:00] life's.
Improve your health span. My money is not on the supplement.
Dr. Brighten: Well, I think it's interesting too because you raise what a big industry this is, and there are people who gravitate towards supplements because they feel like, okay, well pharma bad, I'm Antip Pharma. Not realizing that pharma actually owns the most profitable supplements that you can buy in the United States and so clever on pharma.
We'll give them that. But I think sometimes people think like. Well, if it's natural, then it's just better. Um. I would love to hear your take. You know, medications, nutraceuticals, natural is more better. Is that what people say? But they say natural must be better. What are your thoughts on that?
Mary Pardee: Yeah, this app appeal to nature fallacy and um, and I didn't know about this all the time, so I became a naturopathic doctor and it was one of the things that I was interested in is should we stay more natural?
And at this. Point in my career after reviewing everything like natural does [00:04:00] not mean better. And we know that intuitively, right? We have poison ivy, do we wanna eat that Because it's natural? Absolutely not. And then we have things that are synthetic, like you can, you can even look at some prescription medications that are potentially going to improve your health.
Span and lifespan. And so, and then people that are anti pharma, you don't have to think of medications as the opposite one, but would you say that whey protein is good for you? There's no whey protein tree out there. It is processed. We have to do a lot of things to get it, and yet most people would say, yeah, that might be beneficial for your health.
And so we have to really start to question things beyond this Natural is better because I think that one has. Already gone by the wayside, and it's just not what's gonna be helpful in terms of evidence-based medicine.
Dr. Brighten: Mm-hmm. And I think people also need to realize that there are some things that are natural that pharmaceuticals have then standardized.
Mm-hmm. So, you know, there's a lot of times where people will talk about willow bark, you know, versus [00:05:00] aspirin, or you're talking about some cardiovascular medications and it's like. Sure you could get a tincture of these things, but it's not standardized. And when you need a therapeutic dose and you have to know that somebody's in a therapeutic window and actually understand the peaks and the troughs of that medication, it's really important to have something standardized.
So sometimes we iterate on what is natural and improve it for the use of medicine. And I think, um. You know, as somebody who likes to live every day and takes a thyroid medication so that I can do that, um, you know, there's times that people say to me like, oh, well you must be antip Pharma because you studied naturopathic medicine.
And I'm like, I studied naturopathic medicine because I wanted a foundation. Nutrition, lifestyle, the things that don't require me for you to be healthy. And also the training in pharm pharmacology and on having prescriptive rights and being able to support people in those ways. So I'm like, you know, back when, 'cause I, I'm older than you, I'm back.
When I was in school, there was no functional [00:06:00] medicine. There was not like these, um, there nobody was a, you know, this integrative doctor that was actually practicing lifestyle medicine. There was no board certification. This was the only path. If you wanted to be that holistic practitioner who was like, I understand the utility of a dietician and I will definitely leverage them.
Mary Pardee: Yeah, and you, that's such a great point in terms of a lot of the medications we use today are derived from natural products, and we have just isolated the thing that we know works and we've gotten rid of all of the things that could potentially cause side effects and made it so it's standardized in terms of dosing, if you look up.
For instance, statin medications. People will come to me and they're on red ye red rice yeast, and then I wanna switch them to something like Crestor and they'll say, well, why? This is natural, it's better. And I'll tell them, well, there's a bunch of reasons, but the Crestor is going to work better to lower your apo Lippo Protein B.
It's a synthetic, we see less. Side effects with Crestor versus some of the non-synthetic versions of statins. And so [00:07:00] that ability to have and and know the exact dose and purity of what you're taking over time just almost guarantees you're gonna have better effects. And we have so much more research around these things as well.
Mm-hmm.
Dr. Brighten: People get. Afraid of statins because of the side effects, but there are ways to help mitigate that. What do you talk to your patients about?
Mary Pardee: Yeah. Well, the first thing I say is that statins are one of the most demonized medications that we have out there for some reason. So social media took hold of them.
Podcasts have taken hold of them, and I think a lot of the side effects that they talk about are unwarranted. If you exercise a lot, you have potential side effects of. Tearing a muscle, right? Getting injured, but we would never tell people, don't exercise because those side effects exist. Everything that we do and enter.
Enter into our life is gonna have potential side effects. It's all about the risk benefit ratio. And when it comes to heart disease, heart disease is the number one cause of death. And A-S-C-V-D atherosclerosis plaque formation on the [00:08:00] arteries is completely preventable with what we know right now. And so because it's such an important thing, those benefits start outweighing potential risks pretty heavily, especially when we have.
So many different therapeutics now to lower A POB levels that we're not reliant just on statin medications. If somebody doesn't tolerate statins, first of all, they're, they're idiosyncratic, meaning that somebody may not tolerate Lipitor, but they do great on Crestor, and so you just need to know how to move around them.
Change dosing. You can even do every other day dosing, and then you can go to other classes of medications if that's not working for somebody. So we've got edic acid, we have Zetia, we have PSK nine inhibitors. Um, we can talk about lifestyle as a piece of that as well. We now have these RNA medications, so there's just so many different options that it doesn't have to stop at statins, and I think we need to be more open-minded about it.
There was a research study that was really interesting that. Took people who said that they have, um, statin induced myalgia, muscle pains from statins, and they [00:09:00] did a placebo control with them where at one phase they gave them the statin. At the other phase they gave them placebo. They didn't tell them, and then they swapped within the same group.
And what they found is that the people that actually had myalgia from the statin. They would only get the myalgia when they were taking the statin, but they should not get it when they took the placebo. And what they saw is that it was a fraction of the people who complained that they had this statin induced myalgia actually had it.
So a lot of this is like the nocebo effect that's going on as well. Mm-hmm. And there's, and there's a real thing.
Dr. Brighten: Yeah. I wanna talk more about, you know, heart disease and because when we talk about longevity, it's not just like. How do you live longer and look healthier? It's also how do you prevent these number one killers, which, especially in women we know not only is heart disease, why are we not talking about heart disease more in women?
Like we, we get a whole month to breast cancer. Important. Mm-hmm. However. It's heart, heart [00:10:00] disease that's going to get us, and it's often medicine who's gonna miss us because we present differently. So I definitely wanna talk to about that. But I did wanna ask you, 'cause we started talking about supplements.
Are there supplements that you think are truly worth it for longevity? Especially when you're layering it on the framework of great nutrition lifestyle. Like you're doing the right things already.
Mary Pardee: Yeah, there's some that are interesting to me that I'm keeping an eye on. Um, for me, I think creatine is kind of a no brainer.
It has good results in terms of strength, power, outputs. Also some cognitive things like potentially increasing memory and, and just like overall cognitive function. So that's one that I think is, is an easy one. It's cheap. Creatine monohydrate, um, tastes like
Dr. Brighten: garbage most of the time. I
Mary Pardee: don't mind it.
Dr. Brighten: I You, you don't mind it?
I don't like to, uh, I mix it with electrolytes to like get it down, but I always get messages from people that are like, you should just take creatine gums. I'm like, oh, with those
Mary Pardee: tastes? Yeah.
Dr. Brighten: 10 to [00:11:00] 15 grams of added sugar to my day, like. No thank you. Look, why take the creatine then?
Mary Pardee: For some reason, the gummies for creatine tastes garbage to me.
I, my, oh, I'm glad tried
Dr. Brighten: them.
Mary Pardee: Oh. Um, that's
Dr. Brighten: why they have so much sugar, though.
Mary Pardee: I have to probably. Yeah. The good ones probably are loaded.
Dr. Brighten: Well, my friends who are dentists would seriously slap me if they, they knew I was eating gummies with that much sugar. It's sticking to my teeth.
Mary Pardee: Oh, what we do, um. The other one, whey protein has great research to maintain and build muscle.
We're gonna talk about muscle today, I am sure, but muscle is one of the cornerstones for longevity and health span. Um, I think of whey protein as a food, so if you would rather eat chicken than eat chicken kind of thing. I think a lot of people are trying to get in a little bit more protein between meals, especially if you're in more of an anabolic kind of growth phase.
So that can be a helpful one as well. Vitamin DI use just. To get people to a good level. So if they come in and their vitamin D is already at a 50 on their own, and maybe it's even winter time, so we're not even thinking it's due to being [00:12:00] outside for the summer, then I'm not gonna supplement them at all.
We'll just keep monitoring. Um, but if somebody comes in low, then I think supplementing with vitamin D makes
Dr. Brighten: sense. And what do you consider low?
Mary Pardee: Below 40.
Dr. Brighten: Okay.
Mary Pardee: So I want people between like the 40 and 70 ish range, ideally.
Dr. Brighten: Mm-hmm.
Mary Pardee: And um, so vitamin D I'm trying to think if there's any others. There's some interesting ones where it's just like alpha ketoglutarate, I've got my eye on right now.
It's mostly animal data. It's. Kind of interesting, but that's where I leave it. So I'm personally not taking it. I just think that it has a potential to maybe show something. Um, people always wanna know about NAD or nm the precursors to NAD, and that's one of the ones that I think is potentially interesting.
Right now. There's no way I would ever go to a clinic and get an IV NAD drip. There's not even close to the research that I think that warrants that. Price tag. Um, and then why not just do a precursor like NR nicotine riboside, which actually may get into the [00:13:00] cells better and increase NAD intracellularly more efficiently than actually doing an IV drip on it.
But still, the whole NAD NR kind of for longevity and. Span specific groups and populations, I think it's very likely to have some benefits, but for the vast majority of us who are healthy and just wanna live a better, longer life, like, I'm not sure yet. So you can see like I'm really skeptical and there's ones that I'm interested on, but like nothing that's like a home run for me other than the ones that I mentioned in the beginning.
Dr. Brighten: Yeah, it's very interesting to me to see how NAD has shifted. So four to seven years ago. Hmm. NAD IV was really affordable.
Mary Pardee: Hmm.
Dr. Brighten: Um, and when I went through I-V-F-N-A-D was something that I did IV that I also was supplementing with it. I have seen it explode and now seeing the price tag of like $500 for an iv, and I'm like, I
Mary Pardee: here.
Yeah.
Dr. Brighten: What happened? Why does it suddenly cost so much more? Because the demand is there. And welcome to capitalism, the demand increased and now we [00:14:00] see it's, you know, a very, very hot one. Uh, what do you think about Euro lith?
Mary Pardee: Olefins one of the ones that I'm interested in totally interested in. Again, I don't think that there's anything out that's like, yes, home run, everybody should be on it.
It's gonna extend your lifespan. But I think it's an interesting one for like mitochondrial health and things like that. I just need more data to make it warranted. 'cause otherwise you're taking that, then you get into the group, you're taking 20 things that are maybes. Mm-hmm. And, and then you don't know what actually is benefiting you.
So I would rather, and. If you really look at all the data around this, you are looking at like the last 2% of, you know, improvements that you're gonna get if you really wanna move the needle. It's none of this. It's all of the other stuff that we're gonna talk about, which is gonna give you the most bang for your buck, and I'm really happy to get the most bang for my buck and like wait on the few kind of question marks and maybe add them in at some point.
Dr. Brighten: Before we get to that, I wanna ask you about rapamycin.
Mary Pardee: Yeah, rapamycin. Uh, Matt Capline is a colleague and friend. I had him on my podcast. Um, [00:15:00] he's one of the leading experts in rapamycin, and that one I'm really excited about. And that is one that I potentially will take in my lifetime. Um, I'm in my 30 late thirties now, and I.
Think I'm gonna wait closer to like four, mid forties. Um, but rapamycin, I'm really interested on for, because I'm an a OE four carrier. Mm-hmm. So a OE four carriers, we think that there may be a potential increase in benefit with rapamycin in terms of risk for Alzheimer's dementia. Um, and, but yeah, the rapa.
Trials are ongoing. Like we're gonna learn stuff in the next five years about what it's doing in humans in terms of lifespan. But I think it's really interesting, really fascinating. Um, I, when I had him on my podcast, I'm like, what do you think right now in terms of longevity? He goes, we know nothing. And this is the guy that's like the lead researcher, one of them in rapamycin, so.
Mm-hmm. I think it's got great potential. Gonna keep a close eye on it and yeah, I think I potentially, when you think about Alzheimer's disease, the risk benefit ratio changes versus other things, right? Because you, I really don't wanna [00:16:00] get Alzheimer's, so if there's something that I can do that has relatively low risk, even if it's potentially not going to help, I'm more likely to take it versus doing that for like, you know, preventing.
Muscle tear. I'm like, I don't really care about that. Why would I do that?
Dr. Brighten: Mm-hmm. I feel the same like with creatine, coine, like some of these supplements that have potential with preserving brain health. I'm like, you know, well see. I'm older than you, so I'm like, I don't really have time to wait for the research, which is where a lot of my colleagues are at.
So I'll be turning 45 next year. Rapamycin is coming down the pipeline for me because I can't wait on this. Study, right? Yeah. If it's saying it can extend your reproductive years by three to five years, so delaying menopause so that you get more of the brain, the heart, the bone benefit. I have to start this now.
I can't wait for the trial. Yeah. And I do that with informed consent. I have friends who are older than me and they're like, I am already on it, and let's see what happens. I'll be my own end of one it. These things are not without side effects. So I say [00:17:00] this with the caveat of. Informed consent, my own informed consent.
And you need the same thing you brought up, um, A POE. Not a lot of people are gonna know what that is. Can you explain that?
Mary Pardee: Yeah. A POE is a genetic marker for Alzheimer's disease. And so you get one copy of your A POE from mom, one copy from dad, and from each of them, you either get a two allele, a three allele, a four allele, and each of those confers either less risk neutral.
More risk. And so the APO E four allele is the allele that has an increased risk for Alzheimer's dementia. And if you have one copy, it increases your risk a little bit. If you have two copies, meaning both mom and dad gave you the APO E four, your risk is much higher. Now, if you have two copies, it does not mean you get Alzheimer's disease.
There's many. People with two copies who won't get Alzheimer's disease. So it's not a deterministic gene. Um, and we wanna say even if you have one, but especially if you have two, we're doing [00:18:00] all of the other things that we know to reduce your risk from lifestyle, because lifestyle is going to be a huge component of risk for dementia.
Dr. Brighten: So speaking of life, lifestyle, let's get into how does muscle actually affect how long we live?
Mary Pardee: Muscle, I think is, we're not talking, we're talking way too much about supplements, not enough about muscle, and that's what I was,
Dr. Brighten: but seriously, we, we had to start there because like that's where all the hype is, right?
Mary Pardee: Totally.
Dr. Brighten: It's one thing, and to be fair, as one of two countries in the world where pharma is allowed to advertise to us, we have been conditioned by watching TV at least, you know, when I was younger, the ads were always running. We didn't have streaming channels to negate that, of saying here like. This pill.
This pill? Yeah. This pill. Yeah. Yeah. Like, you know, she's running through the field with balloons and she's so happy 'cause this pill. And so I think it's really shaped our mindset and what we have to do is start reminding people that so much of what will actually move the needle is what you do every single day.
Yeah. [00:19:00]
Mary Pardee: And that's why I love our profession too. Lifestyle is like the cornerstone. Um, so muscle plays a really important role in the body, and people think of it as a structural kind of tissue, which it is, but it's much, much, much more than that. It's very active metabolically, and so the amount of muscle you have on your body increases if you have more muscle.
It increases your basal metabolic rate, how many calories you're actually burning at rest. Also increases fat, oxidation, muscle secretes different things from it as well. So it's very active. It, it puts out things called mykines and we have anti-inflammatory MIT mykines that are cardioprotective for our heart.
We have things that are secreted that reduce, um, tumor necrosis factor alpha, which is an inflammatory cytokine. Um, and we have things that will actually, like, um, there's one called Irisy that's released from the muscle that is, um. Anti-neoplastic can reduce. Certain types of cancers. And so we have all these things coming from muscle [00:20:00] that are much more than just structure, but actually improving our insulin sensitivity and muscle acts as this pump when we're walking or when we're lifting something.
And the actual contraction of the. Can help with something called insulin, independent glucose uptake. So that is when you get sugars in your blood and it goes into the muscle cell, takes up and doesn't need insulin to unlock that cell to let it in. So typically insulin has to be around to let sugars into the cells.
Um, but exercise alone acts as a different way to get those sugars in. So reducing your risk. For insulin resistance, pre-diabetes, diabetes. And then we also know that muscle helps with, um, nitric oxide signaling to improve our endothelial function of the inside of our arteries to reduce the risk for heart disease and things like that.
And then if we just start to look at the stats behind. How much muscle [00:21:00] somebody has on their body and what it actually does long term. So if we look at one end of the spectrum, we've got sarcopenia, people with low muscle mass, and people with low muscle mass have a 60 to a hundred percent higher risk of mortality.
Mm-hmm.
Mary Pardee: With sarcopenia 60 to a hundred percent higher risk of mortality. It's not a little bit, these, these are huge numbers. They have longer hospital stays. If something happens, they stay sick longer. Um, if somebody is diagnosed with cancer and they had sarcopenia prior to being diagnosed, they have a 49% higher risk of mortality from that cancer compared to if they had normal muscle mass.
Beforehand. And so muscle matters. It is making sure that we don't fall. It's making sure that we actually can shower ourselves by the time we're 80, 90 into our hundreds as well. And then this all plays a role when it, when we talk about, um, osteoporosis, because if you have low muscle mask or wrist for [00:22:00] osteoporosis is three x what it was.
So it triples and it's about one in two post-menopausal women will have an osteoporotic fracture at some point in their lives. That's one in two, that's 50% of women. Huge,
Dr. Brighten: huge,
Mary Pardee: huge. And um, and we don't wanna break a hip. So if you look at the stats around hip fractures, and we'll just look at women. If you're 70 years old and you break a hip, 5% of those women who break a hip at the age of 70 will be dead within two years.
If you're 80 years old, you break a hip and you're a woman, it's about 11%. That's one in 10 of those women will be dead within two years. And if you are a. 80 plus years old and you break a hip, it's about 26% of those women will be dead in two years. That's one in four women. So really high mortality rates with hip fractures because of the things that follow it, um, but really emphasizes why it's.
So important to be strong as we [00:23:00] age, so. Mm-hmm. That's one of my main things is like, how do we age stronger? How do we get people to avoid frailty in a really graceful way?
Dr. Brighten: Yeah. You know, as you're talking about this, it, because I just recently had a knee surgery, which was a freak accident of a piece of cartilage just coming off my knee.
Like I did nothing fun to do this. I probably did something in my twenties that like set me up for this. Mm-hmm. But I was, as soon as I woke up. From surgery, I like open my eyes and the first thing is that I'm lifting my legs. I'm doing all these exercises, I'm pulling, I'm moving my knee, and the nurses are like, no, no, no, no, no, no, no.
We don't want you moving at all. And I'm like, you don't understand. You do not understand. And when I saw my physical therapist and my, uh, surgeon following up, they were like, I was telling him like how the nurses were telling me no. And they're like, so good that you did that. Like, we're so, and I'm like, yeah.
And, and you know, they're, they're trying to be encouraging to me 'cause I'm like, I have to keep working out. And they're like, no, you could take three weeks off. And [00:24:00] I'm like. I'm 44. That's a lie. Like I can't, I can't take those three weeks off. But I think, um, you know, when you, uh, start to understand this stuff.
You are start to understand like what the risk is. You can be empowered to take action. So if somebody's listening to this right now, often when we talk about how important muscle is, they think, oh, I have to be a bodybuilder. Like I like, I have to be like. Extreme right, because that is what the algorithm on social media often, you know, serves up.
Or you're in the age group where like Arnold Schwarzenegger was a thing in your life. What can women do that's an actual step daily to start preserving and building muscle mass?
Mary Pardee: Okay. I love this question. Can I reverse a little bit though? I, I wanna like set the stage in terms of, I think people don't understand women with exercise I think is a really important topic.
Do you know who exercise is? More men or women?
Dr. Brighten: I would assume it's women and doing cardio.
Mary Pardee: I said the same exact thing. And the answer is [00:25:00] that women exercise less than men at every single stage of life.
Dr. Brighten: Dang.
Mary Pardee: I know.
Dr. Brighten: I don't know. See, I was a group fitness instructor. That's how I earned money through college.
So,
Mary Pardee: so in
Dr. Brighten: all my classes, classes are women. So I would just assume that like, of course women are always at the gym, but wow,
Mary Pardee: I, I have the same thing. Women exercise less. Than men in every single stage of life. So if you look at women in their fifties to sixties, about 18% of women meet the American Heart Association's recommendations for aerobic and resistance training.
18%,
Dr. Brighten: which is also a very low bar.
Mary Pardee: That's so low.
Dr. Brighten: Like it's a, it's a low bar of
Mary Pardee: movement. Oh, what, what the thing is?
Dr. Brighten: Yeah. What the requirement is isn't like something extreme.
Mary Pardee: It's 150 minutes of aerobic activity. Yeah. With two days of strength training and only 18% of women 50 to 60 meet that requirement as we age.
Less and less people meet that requirement. So as we age every single [00:26:00] decade after our teens, fewer and fewer percentage of people, both men and women, will meet that requirement. And so when people are talking about, I don't wanna over exercise, I'm like, don't worry about it. Like there's a group of people that are doing it, but it is such a small percentage of the population is over exercising.
The vast majority of people are under exercising. And I'm like, come on ladies, like we gotta at least meet these men. Um, and so resistance training is so important for women. I think that it's gotten marketed to men and it's gotten marketed that you're gonna get bulky and you're gonna have these big muscles, and women should more do Pilates, or they should be on the treadmill or the elliptical, and it's done Women such a disservice because mm-hmm.
Women need resistance training. In order to maintain health, I think people think that health is given to you. Health is earned.
Dr. Brighten: Mm-hmm.
Mary Pardee: And this is one of the things that you have to do to, to earn that piece of health. Um, women have much higher rates of osteoporosis than men do, and the resistance training is one of the [00:27:00] number one things to do to both prevent and treat osteoporosis.
We also see that women who exercise regularly have a 22% reduced risk for breast cancer. We see people that have higher grip strengths have a reduced risk for almost every single type of cancer, cardiovascular disease, dementia, you name it, it's on the list.
Dr. Brighten: Mm-hmm.
Mary Pardee: Um, but it's so, so important. And so when people come in and they, they come to me and they're doing, like they're doing one day at Orange Theory, and then they're doing one day a Pilates, and maybe they're doing like a run kind of thing.
I'm like, okay, that's great. Any movement is better than no movement at all. But we wanna separate this into aerobic versus. Resistance training. 'cause you get totally different benefits from both of them. When we talk about resistance training, the plan should be really simple and that's just, just start lifting weights and then write everything down.
And then every week make sure that you're increasing the weights, you're lifting or the repetition so your volume is increasing and just do it really methodically. But start. [00:28:00] Slow, go low, but push yourself to a place that is getting harder and harder and harder. So I sit with all my concierge patients. I just did this yesterday.
I take out my training log and I'm like, this is what it's gonna look like. And we get into the weeds of it. 'cause it can be so simple and effective if you're doing it the right way. But most people, like I said, are just kind of throwing stuff at the wall, hoping something fits, doing all this random stuff versus having a progressive overload plan.
Dr. Brighten: I am so glad we're having this conversation because I have shared with my audience multiple times that I call it how not to die protocol. And anytime I'm like, Ooh, I don't feel like working out, I'm like, do you feel like dying?
Mary Pardee: Mm-hmm.
Dr. Brighten: No. Oh, I don't feel like going in my sauna. Like it's uncomfortable sweat.
It's gonna take time. Do you feel like dying? No. Okay. Like, and that's something that I check in and, but people have come in like. That's morbid. That's not a good way to think about it. And I'm like, if you know the research, the research you just laid out, you can't unknow it. You can't unknow it. And when you look at what is coming down the [00:29:00] pipeline, it's how I've always practiced medicine is I look at my patient, I look at what their goals are right now, and I try to be predictive of what's gonna try to take them out in the future.
Mm-hmm. And that's where we have to focus. And for women we know. It's gonna be osteoporosis, but cardiovascular disease, so we've got dementia. We're like 60 plus percent of that population. Mm-hmm. But we've got cardiovascular disease. So I wanna talk to you about this concept because people often think like, I'll just take statins when I get there.
What is more powerful in your clinical opinion when it comes to preventing heart disease? Waiting for the statin or coming in with the lifestyle?
Mary Pardee: Both. I don't choose between these two things 'cause they're very different in my mind. Mm-hmm. These are two different things. So we know that A-S-C-V-D is preventable and is caused by elevated levels of Apolipoprotein B containing particles.
Like LDL is what we talk about the most. Um. If we take away that as a [00:30:00] potential cause, so if we lower your APO lipoprotein B. If you look at the piece of trial, they looked at LDL cholesterol levels at 50 0% of people in that trial had plaque formation in their arteries when their LDL was 50 or below. We should use that information.
And so I get all of my patients to have an LDL of around 50 to 60. I measure a OB. So again, I keep it around like the 55 for apolipoprotein B. Um, and then that's that. And that may be using diet. So if somebody comes in and their, maybe their LDL is like. 65 or 70, then we may be able to just reduce saturated fat in that person's diet.
Reducing saturated fat in the diet gives you about a 20% up to a 20% reduction in LDL cholesterol levels. If you're eating virtually no saturated fat, you're not gonna get a 20% reduction. So this is people that have it in the diet and are able to take it out. Um, some people, if you come in and you're eating super high saturated fat, maybe you're on carnivore or keto, then you might be get a, a little bit bigger of [00:31:00] a reduction there.
But LDL and apolipoprotein B are so genetically linked that there's not a huge lifestyle component to them. Mm-hmm. And I think we really need to sit with that because people think they have control over everything. You can't change your A POE for. Alzheimer's. You don't have control over that, and you don't have total control over your LDL and APA lipoprotein.
B. You have some, but not as much as you, you may hope and think. And so that's where medications come in is just to get people to that goal unless they're already really low to begin with. Now, the lifestyle things I said are separate because you get additional risk reductions with starting to exercise.
So if you start to exercise, say you're exercising like 300 minutes a week, you get a 22% reduction in your risk for coronary artery disease. That's incredible. I wanna compare that to though the person that comes in with an LDL of 140 that we lowered their LDL to like 60, that person has an 85 plus percent reduction in their risk for heart disease.
Dr. Brighten: Mm-hmm.
Mary Pardee: It's not that they don't do the [00:32:00] exercise 'cause they should get another 20% reduction, different mechanisms. So heart disease in terms of exercise, exercise on a regular basis reduces your blood pressure. We want that regardless of what your apo, lipoprotein B is, it helps with endothelial function and nitric oxide synthesis.
We want that in terms of heart disease and so I really push people, this isn't an either or kind of thing. It's a yes and mm-hmm And sometimes we don't need meds, like I said, like I've got those people that come in and naturally their a OB is. 55 and they've got great genetics and then they don't need a medication.
You just monitor.
Dr. Brighten: Yeah. And I think the other thing that people need to understand the context of this conversation is that your cholesterol, your blood pressure, everything may have been fine your whole life and you go into menopause. And now that's a different story. And I don't think women are being monitored enough and closely enough.
I also had the experience of, um. So my second child was born at 40 and at three months postpartum I was like, I wanna get a [00:33:00] full workup. I wanna check my thyroid, I wanna check all this stuff. And then the first time in my life I had elevated cholesterol and my doctor was like, hold up. Like this is very concerning.
She's like, what is going on here? And I was like, I'm postpartum and 40, I have no estrogen right now and I'm breastfeeding. And she's like, wait, say more. And we have to have a whole conversation. 'cause she was like, I don't. Ty, I'm not treating like, I'm not doing any kind of menopause care with hormones.
And I'm like that. And, and it was a, a big aha moment for me of like, okay, wow. Like this is for shadowing. This is the things to come. And I think, think if any woman's listening to this, she's ever had high cholesterol in her life, she's had high blood pressure. She's had any cardiovascular risks, pay attention to this information closely because once you are in menopause, all of this better be monitored and checked and you can always go on estrogen therapy.
That significantly helps, but it's certainly, I think there's a huge disservice being done to women right now with the whole menopause conversation always being about hormone therapy. And I'm like, [00:34:00] okay, I've been prescribing for over 12 years. I'm a big fan. Okay, love, love hormones when they're indicated.
It is not enough. It is not enough.
Mary Pardee: Yeah. Yeah, yeah. If you, if you come in with an, uh, an LDL of like 1 35 estrogen's not gonna get you to optimal ranges. It may improve things, but it's not gonna get you to optimal ranges from what I've seen in practice. Um, and then for the women who are younger than. The perimenopausal menopausal age group.
I have women come in in their twenties and thirties. If you come in in your twenties and thirties and you do all of this stuff, you can improve your health span and lifespan substantially. 'cause you're at a such a young age. Mm-hmm. But what I've noticed is that these people come in, they have, like, I had one woman.
20 something years old, LDL of 1 35. And I'm like, has anyone else told you to go on medication? And she goes, no, I'm too young, they say, and that is something that you hear all of the time from other doctors', primary cares that oh, they're their 10 year risk for [00:35:00] cardiovascular diseases. So low 'cause they're so young, so we're not gonna treat them.
Now that makes. No sense to me at all because we know plaque formation in the arteries is all about how much time LDL has been exposed to those arteries to create damage. So why would you give it 10, 20 years to do damage when you can just. Stop it in its tracks at the age of 20 and never have exposure to the those arteries.
And so I treat women as soon as they come in, in their twenties and men, um, and get them to optimal ranges so you don't have any plaque formation that's going to happen. I don't care if you're not gonna die in 10 years. I'm like, yeah, I don't think she's gonna die by the age of 35. I also don't want her to die by the age of 85 by a heart attack.
And that's how you prevent it.
Dr. Brighten: Mm-hmm. So people will often present the argument that cholesterol does not matter. If there is no inflammation in the body, what do you say to that?
Mary Pardee: Yeah, that's a common one that goes around social media and it's just completely false. So you can have zero, like you can have [00:36:00] completely normal CRP completely normal SED rate levels, and you can still put plaque down in your arteries.
It's not an essential component. Now, if you also have inflammation, could it. Speed things up. Absolutely. You know, that's why one of the reasons potentially that obesity can accelerate A-S-C-V-D plaque formation. Um, but if you have a really low A POB, you can't put plaque down. And so I, someone just commented on Instagram the other day, they're like, you're so reductionistic.
It's not just about a OB. I'm like, I'm not saying it's, I'm the person that's talking all about lifestyle, all about nutrition, all about exercise. And let's not forget about this piece that's causing a good chunk of this A-S-C-V-D and just treat it.
Dr. Brighten: I'm gonna be honest, I think people who say that it's because they don't actually have a deeper understanding of the research and the clinical experience that you do that they think you can just out eat it.
You can just out exercise it. And what I'm hearing from you, yes, nutrition, lifestyle. [00:37:00] Absolutely essential, absolutely important. But there are certain situations and definitely genetic carriers that it's not going to be enough for them. And I think it's really important for people to understand this is very individualized and nuanced and unfortunately no clickbait, um, for the algorithm to wanna share this with everyone.
So we're gonna, we're gonna need you guys to help us share it because it's, if it's not. Sensational. If it's not like, oh, this one thing fixes everything, right? The algorithm doesn't serve it up, and it's such a disservice. I think we're gonna have a study in the next 20 years of how social media. Training people.
Right. Because even doctors have to say things sensational and then you try to get into the nuance. But how, what the impact of social media was on people's health. Mm. By not serving them the actual information that would've helped them.
Mary Pardee: Totally agree. Totally agree. Yeah. Yeah. It's something that we need to, and it, it just starts with each one of us.
Right. But I get it too. 'cause I also have an Instagram following.
Dr. Brighten: Yeah. I mean, I think everybody gets it these days. Who [00:38:00] creates content and you're like, this is so good and so educational. And the algorithm's like, well, we'll show this to no one. And then, right. Yeah. You're just like, you say something like off the cuff and then it's like, oh God, I didn't get to say all the nuance.
'cause it was a seven second clip. And that brings everybody, everybody wants to see it. Let me ask you. What's your take on why people gain weight as they age? Some people say it's metabolism slowing. Some people say it's just your hormones changing. What's the big picture of what's happening?
Mary Pardee: I did this in a talk and didn't go over well with the crowd, the crowd, but so from the ages of 20 to.
60. Our metabolism does not slow. We know that now. So ages of 20 to 60, your metabolism stays the same. So when women come in in their forties, fifties, or men and they say, oh, I'm just getting older. My metabolism slows. I'm 45. I go, I'm so sorry. It's not because of that. Let's take that off the table and actually empower you with the things that are going to help because you can get great results for weight loss.
Um, after the [00:39:00] age of 60, we see, we see minor declines in metabolism, but you're looking at 0.7% per year. Little, little bits, not these huge drastic shifts that we think now what we do. A hundred percent know that changes as we age is what I talked about before, which is exercise. So every decade of life after your teens, people, both men and women, are exercising less and less and less by the age of 50 women.
About 18% of women are meeting those minimum requirements from the American Heart Association for Exercise. And so I think that it's two part. I think that it is, we are not exercising enough and I think that we're. Eating more, and there's hormonal shifts that can contribute to increase cravings and appetite.
Mm-hmm. And there's medications that can increase your appetite. And the fact that we live in a, a world that has so much ultra processed food at every single corner, the accessibility, um, I think plays a role in it as [00:40:00] well. But I think that it's. Those are the things that we should be focused on versus, you know, trying to find like this like hidden kind of thing.
Dr. Brighten: Yeah. I would also add that, you know, we know as estrogen goes down, we can accumulate visceral adiposity that can lead to increased inflammation, insulin, insulin resistance, and that can shift our metabolic health in a negative way. And for people listening. Yes, estrogen therapy is an option, but we also know what moves the needle there.
Higher fiber diet, less added sugar, which is what you were talking about with the ultra processed food. Ultra processed food is like, it's like eating styrofoam sometimes, right? But it tastes better where you're just like, you're getting no fiber, no nutrients, nothing from it. And I'm not here to be like, never eat ultra processed food because it's just not.
The society that we live in. But it is to reflect on that as well. 'cause I think that you are right as well, that hormones shift [00:41:00] cravings also shifts satiety. So your sense of feeling full. So there's a lot of factors going on here and. But it's also, I think, why women feel frustrated when people are like, just eat less and move more.
And it's like, that's so easy to say. You're acting like I, I, it's a willpower issue when it's like I've got a whole physiological shift happening here that's working against me.
Mary Pardee: Totally. And maybe you're a mom of three and you're running to soccer practice and juggling your own career, so. I'm not saying any of these things are easy, but I wouldn't put my time towards like some of the kooky things out there for weight loss.
I would put my time towards how can I make sure that I can have a better diet and maybe I do need to go on hormone replacement therapy to help with my mood or, you know, whatever it is, kind of thing. Get all the foundations in place, but absolutely estrogen dropping. Um, re, re shifts. Fat dis distribution.
Right. So hormone replacement therapy doesn't cause weight [00:42:00] loss, but it can change fat distribution in the body away from the midsection down towards the hips, foot and thighs, where it doesn't increase the cardiovascular disease risk as much.
Dr. Brighten: Mm-hmm.
Mary Pardee: Good point.
Dr. Brighten: Yeah. I wanna ask you, what's one thing about longevity that you wish people would stop obsessing over?
Mary Pardee: There's so many things. Um, it's the quick fixes. It's, it's the people that are, you know, they're doing the greens powders and the colostrum, but they're borderline sarcopenic. Um, it's, you know, going in for the NAD drip when you haven't exercised in two years, or, you know, it's like doing. It's the minors over the majors.
Mm-hmm. It's like the people. And the influencers that are focusing on these minor things that may have zero evidence or very little, versus the major things that are gonna give you 90 plus percent of the actual effects.
Dr. Brighten: I wanna ask you about GLP ones because you said quick fixes. A lot of [00:43:00] people see that as a quick fix.
However, in the context of the conversation, we've been talking about weight loss, but now we're starting to see really promising trials for cardiovascular disease coming out. And, uh, starting to look at Alzheimer's and dementia patients as well. So from a longevity perspective, we're starting to see there's the people who write.
We started with GLP ones because they needed weight loss support or diabetic, but we're starting to see a lot more people using them at lower doses because of the potential cardiovascular and. The cardiovascular is actually established, so I won't say potential, potential for the individual, but the cardiovascular outcomes are established.
The brain is the one that we're like still waiting for some more robust data to understand that. But what are your thoughts?
Mary Pardee: Think kidney function we're seeing as well? Yeah,
Dr. Brighten: kidney function.
Mary Pardee: Um, I think GLP ones have a potential to be a jero protective, meaning like a longevity drug. I think it's a potential.
So we need to start looking at them more in normal weight individuals. Seeing [00:44:00] health outcomes in those individuals and can we use them in normal weight? Individuals that doesn't induce osteoporosis, like too much weight loss. Right. So is there,
Dr. Brighten: thank you for saying
Mary Pardee: it. Is there somewhere like a happy medium where we can get some of these potential effects without, um, negative side effects for those normal weight or healthy weight Individual?
So I, it's one of the ones I'm really excited about in terms of potential Jarrow protectives. Would I go on one right now? Self with that in mind. Absolutely not. Like my risk of osteoporosis, sarcopenia way out if I lost weight or muscle way out weighs potential, um, benefits. And so we gotta figure out like dosing what that looks like and if we, if we're getting the same effects with normal weight people as people who are overweight.
Um, but I use GLP ones in my practice all the time with people where it's indicated and going to be helpful and in conjunction with resist. Training and all the things that we've been talking about, the outcomes are incredible. And you mentioned something before where it's like, well, of course, just. [00:45:00] Eat less, exercise more.
There's a lot of people who have been trying that for a long time and they lose 10 pounds and then they gain the 10 pounds, they lose 20 pounds, they regain it. And this is a huge step for obesity medicine because we're seeing people lose the weight, lose more weight, keep it off, and their mental health is changing.
Mm-hmm. So the, the number of people that come into my practice and they, they've only lost like the first 10 pounds and they've got a hundred plus to lose, but they're like. I've had people crying in tears, just being like, I have my life back, because they're not thinking about food 90% of the day.
Dr. Brighten: Mm-hmm.
Mary Pardee: Um, so there's so many aspects to obesity and there's a huge obesity bias in our, in our country, and we really have to view it as more of a disease state that has many different layers to it. One of them is mental, emotional, and appetite regulation and all this other stuff.
Dr. Brighten: Mm-hmm. I appreciate you though.
Bringing up the muscle loss, the sarcopenia, and the, uh, [00:46:00] osteoporosis risk because I had people asking me to do a GLP one episode and talking about the science of cardiovascular disease and the potential benefits and pairing it with HRT and how all of that works. Suddenly, I sent that episode was if you lose weight and it is muscle.
You are not healthier. You are just smaller. The number of women I had, right, who were like, I've been going to a med spa getting these GLP ones and I am losing muscle. Like, it never occurred to me that smaller doesn't mean healthier because the healthcare practitioner prescribing this didn't actually do a, you know, body analysis, didn't do a Dexa Omni, didn't do any of these things to make sure that like this was the best move for me.
And so. I just really wanna underline what you're saying because I think, you know, it goes back to what the exercise piece of what you were saying of women being told to do cardio, do Pilates, right? We're constantly told to shrink ourselves and that's [00:47:00] been packaged as health. But from this conversation for people to understand, I want you to go rewind and listen to what you said about sarcopenia and and osteoporosis risk, because you're absolutely right.
Shrinking your body. It isn't gonna necessarily mean you're healthier and it may put you at risk for the things that we are actually dying of. Yeah.
Mary Pardee: And I'll add one more layer to that, where if you have somebody who's indicated for these GLP ones, they're overweight, they're obese, they have weight to lose, it's affecting their metabolic health.
Um, the weight loss percentage from lean tissue versus fat mass is no different than if they were to do lifestyle changes. So we see the same amount of muscle mass loss with GLP ones as we do with lifestyle changes, um, throughout the trials, which is about like 25 ish percent of the weight loss will be from muscle mass.
I measure that in all my patients. And so I just had somebody that come in, oh, your percentage of muscle mass loss versus fat loss is a little higher than I'd like to see it. Like, let's really focus on the resistance [00:48:00] training. Um, but you, you will always lose muscle when you lose weight. That's just where my concern comes in with normal weight.
People that we're not trying to lose weight, we don't want. Uh, muscle losses in them.
Dr. Brighten: Yeah.
Mary Pardee: Yeah.
Dr. Brighten: Let me ask you, if you could challenge the audience to, like, over the next seven days, do this one simple thing to improve your health and longevity, what would you challenge people to do?
Mary Pardee: Oh, does it have to make them feel different in seven days?
Dr. Brighten: No, but it can start changing their life in seven days. Okay. Because habits, they took time to to, to form. We all think we can just like start doing something the next day and then we'll be with it.
Mary Pardee: I want you to start logging your workouts. This is one of the things that I think has made the biggest shift for my patients is log your workouts in terms of how much weight you're lifting, how many reps, and how many sets you're doing, and create a program where every week you're just increasing that number, do the same exact workouts.
Three days a week. But that one change [00:49:00] I have seen make the biggest difference in people's body composition, risk for metabolic diseases, all this stuff, because it, it ensures a progressive overloading of the muscle. Mm-hmm. And you'll get results. So many people are just like, just exercising randomly, which is great.
That's better than nothing. But if you're gonna do one thing.
Dr. Brighten: That will change it in seven days. You will absolutely start changing in seven days. Let me ask you, what does, knowing what you know about longevity, what does your fitness routine look like through the week?
Mary Pardee: So I do three days of resistance training.
I log everything. I've got a spreadsheet. Um, and it, it. Improves every most weeks. Um, and then I do at least two runs during the week with my little puppy. And so we do a slow run for 40 minutes. In the last 20 minutes I do a VO two max workout, which is sprint intervals. So like all out for 20 minutes on and off a minute.
Ish. Um, and then I play tennis twice a week and I usually go for at least one hike. Um, and that's kinda like the backbones. [00:50:00] Um, and, and I walk my dog twice a day for at least like an hour each time, so I move a ton.
Dr. Brighten: Mm-hmm. Tennis is one of the. Big longevity hacks when it comes to exercise. Um, so, and people playing pickleball as well.
Yeah. Uh, tends to be so, so good for the brain. I wanna do some rapid fire, uh, questions like with protocols that are all longevity focused with you. So, um, I'm gonna say something and you answer like, top of mind, what do you think? Great. What would you recommend to people? So if someone has weak grip strength.
Mary Pardee: Increase total body strength. You don't have to just increase your grip strength. Research is more about your total body strength. So lift weights.
Dr. Brighten: If someone has a family history of heart disease,
Mary Pardee: optimize your A POB. Get it to like 50 to 60. Um, make sure your blood pressure is perfect. Um, exercise. Eat a Mediterranean diet.
Don't smoke. Avoid alcohol. Sleep seven hours. [00:51:00]
Dr. Brighten: At least seven hours, please. Uh, if someone has gained weight in midlife
Mary Pardee: caloric restriction, number one, get about 1.8 grams per kilogram of body weight of protein If you're a woman, 25 grams of protein, or 25 grams of fiber, if you're a man, like 35 grams of fiber per day, and just start moving your body more and more.
Dr. Brighten: There are people who say more is better with fiber. You just said 25 grams of fiber. There are people out there saying, no, women, you need to get 35 to 50 grams of fiber. What are your thoughts on that?
Mary Pardee: I think you need to start low. Go slow with fiber, or you'll never eat it again because it'll cause intense gastrointestinal issues.
So most people, I do diet logs with all my patients. They're coming in at around 10 grams of fiber, seven grams of fiber. If you went up to 35 from there, you would kill me. Yeah. So you wanna gradually increase, just keep adding servings. But 25 grams for women is the minimum, and then it's. Um, it's based on how much food you consume too.
So if you're a woman who's 170 [00:52:00] pounds, you're closer to 35 grams and yeah, more may be better. I don't think that there's really an upper limit for vegetables unless you know, some TikTok or is gonna show me that they died 'cause they ate like two a million pounds. 'cause people do eat things.
Dr. Brighten: It's like whenever people are like, I can't eat broccoli 'cause I have thyroid disease and I'm like.
You know, your gut would stop you before you could eat the amount of broccoli it would take to affect your thyroid. Like we're talking about pounds of raw, raw broccoli. Your gut will say no before your thyroid even knows what's happening.
Mary Pardee: Someone's gonna do it.
Dr. Brighten: Someone's gonna do it now and they're gonna be sad.
Don't do it. And what do you say to someone who's like, I cannot get quality sleep.
Mary Pardee: Uh, I've been there. Cognitive behavioral therapy for insomnia.
Dr. Brighten: Love it.
Mary Pardee: Google it. Find a practitioner and you will send me a thank you note and some flowers because that shit works.
Dr. Brighten: Yes. I, I agree. When
Mary Pardee: you're like, like sleep restriction.
Yeah,
Dr. Brighten: yeah. When you're like, I've done all the sleep hygiene things [00:53:00] and they don't work. Oh, CBDI like works like a charm. If someone's worried about dementia.
Mary Pardee: Um, top four risk factors for dementia that accounts for 30% of global dementia cases is gonna be number one. Um, a sedentary lifestyle. So exercise, hearing loss.
Make sure that you are checking your hearing throughout life, and if something happens, you need to get a hearing aid to fix it. Um, sedentary lip, uh, blood pressure. So high blood pressure. Maintaining a normal blood pressure is super important. And then education level. So continuing. To learn things, learn a new language, um, you know, listen to podcasts that stimulate you mentally have interesting conversations.
Those are the top four right after that LDL levels that are high in midlife three x the risk for dementia. So get your LDL, your a OB levels lower and then it's all the things that we know. Avoid smoking, you know, eat good food, [00:54:00] Mediterranean diet for sure. Um. Yada, yada, yada.
Dr. Brighten: Yeah. Mediterranean diet is always winning.
Um, and I love that you bring up the hearing loss and people, yes, it is true that magnesium has been shown to help with hearing loss. However, an audiologist is the person to see because you're absolutely right if your hearing is going, get a hearing aid, even if you wanna try the magnesium and try other things, no one says you have to do one or the other.
You can do both, and I think it's a great way to marry those things. If you had to make a bold prediction, what do you think we will know five years from now when it comes to longevity?
Mary Pardee: Interesting. Um, I think we'll have a sense of biomarkers for longevity. Like right now, I think some of the better ones are VO two max.
Your. Appendicular lean mass, how much muscle you have on your arms and legs. Um, things like A1C fasting insulin, just in terms of like risk factors for the big things. But I think that we [00:55:00] may know more about like biomarkers for actual longevity. We have these like biological clocks now that people will say, what's your biological age versus your chronological age?
And right now they're trash. Like I wouldn't even touch 'em. Um, at least the direct to consumer ones. But I think like those may be. In a good spot or something like that, in a good spot that we have more. Easy ways to measure longevity. Um, and then I'm guessing like some, some better like Jro therapeutics where yeah, maybe we have figured out the GLP one thing for extending lifespan or rapamycin has more information around it, or we know about maybe some supplements that are, you know, kind of promising.
So I think we'll have more information on those right now because I don't think we have the information right.
Dr. Brighten: Yeah. Well, thank you so much. This has been, thank you. Such a fantastic and insightful conversation.
Mary Pardee: Thanks for having me. It's good to see you too.
Dr. Brighten: Yeah. Thank you so much for joining the conversation.
If you could like, subscribe or leave a review, it helps me so much in getting this information out to everyone who needs it. If you enjoyed this [00:56:00] conversation, then I definitely want you to check out.