


Endometriosis is often described as a reproductive condition—but for millions of women, it’s a whole-body disease that drives chronic pelvic pain, fatigue, digestive issues, and inflammation that can affect nearly every organ system. In this third installment of the Endometriosis Expert Series, leading physicians and surgeons unpack one of the most misunderstood aspects of the condition: pain. Why do some women suffer debilitating symptoms even when scans appear normal? Why does laparoscopy help some patients but not others? And what actually works for long-term relief?
This conversation dives deep into endometriosis relief of pain, laparoscopy for endometriosis pain, and the treatment of chronic pelvic pain in females, offering insight into why conventional approaches often fall short. The experts discuss how endometriosis pain can evolve over time, from inflammatory pelvic pain to complex nervous-system-driven chronic pain, and why a comprehensive treatment strategy is often required.
If you’ve ever been told your pain is “normal,” that imaging looks fine, or that suppression is your only option, this episode explains what medicine often gets wrong about chronic pelvic pain in females and what women deserve to know instead.
Endometriosis Relief of Pain: What You’ll Learn in This Episode
In this episode, experts break down the complex biology behind endometriosis pain and the evolving approaches to treating chronic pelvic pain in females. If you’ve ever wondered why pain persists even after treatment—or why diagnosis can take years—these insights will change how you understand the condition.
Here’s what you’ll learn:
- Why endometriosis pain doesn’t always match what imaging shows—and why many women are told their scans are “normal” despite severe symptoms.
- The surprising statistic that a significant percentage of women with unexplained infertility are later found to have endometriosis or adenomyosis.
- Why laparoscopy for endometriosis pain remains the gold standard for diagnosis, but still isn’t accessible to many women.
- How chronic pelvic pain in females can evolve over time when the nervous system becomes sensitized.
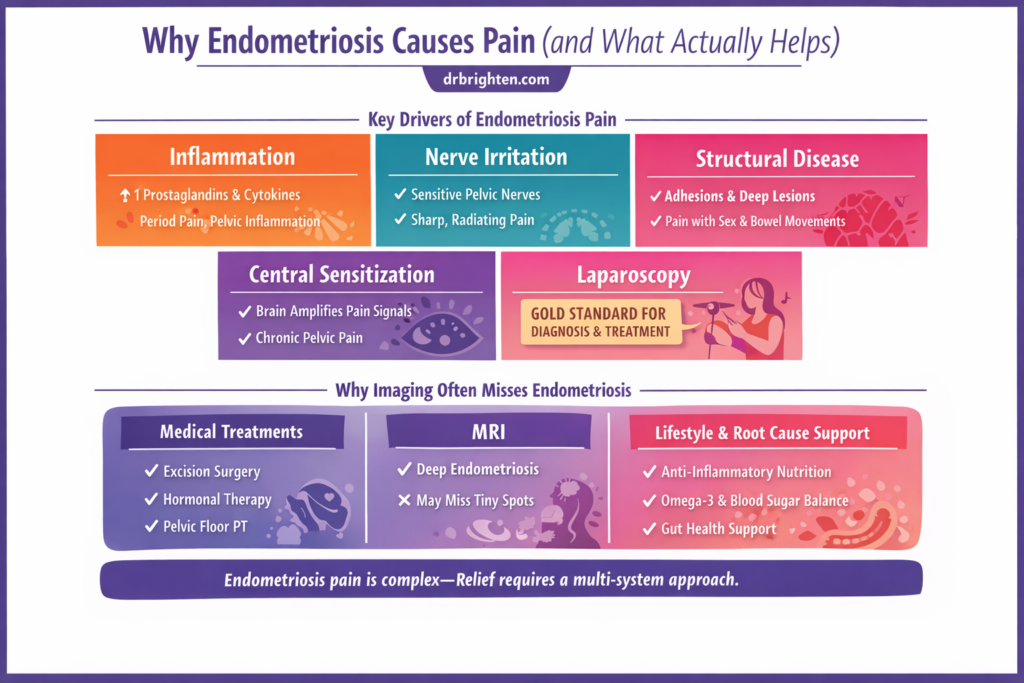
- The difference between inflammatory pain, nerve-driven pain, and structural pain in endometriosis.
- Why some patients experience severe pain even with minimal visible disease.
- The reason many women spend years—sometimes decades—seeking answers before receiving a diagnosis.
- How the body’s immune system, hormones, and inflammatory pathways all contribute to the pain experience.
- Why adenomyosis frequently overlaps with endometriosis and can complicate diagnosis and treatment.
- The role of laparoscopy in removing disease and reducing pain, and why surgical expertise matters.
- Why treating endometriosis pain often requires a multidisciplinary approach that includes more than surgery alone.
- The critical difference between symptom suppression and addressing the underlying disease process.
- The ways chronic pelvic pain can affect digestive health, bladder function, and sexual health.
- Why the medical system has historically underestimated the severity of pelvic pain in women.
If you’ve been searching for answers about endometriosis relief of pain or treatment of chronic pelvic pain, this episode brings together experts who are actively working to change how the condition is understood and treated.
Understanding Endometriosis Relief of Pain and the Treatment of Chronic Pelvic Pain in Females
One of the most important themes in this episode is that endometriosis pain is not one-dimensional. Many women are told their pain should resolve with hormonal suppression or after surgery, but the reality is far more complex.
Endometriosis lesions create an inflammatory environment in the pelvis, releasing prostaglandins and cytokines that stimulate nearby nerves. This inflammatory cascade can trigger intense menstrual pain, pelvic pressure, and pain during bowel movements or intercourse.
However, over time, the nervous system can become sensitized.
When pain signals repeat for years, the brain and spinal cord may begin to amplify pain signals, even after some of the original triggers are addressed. This process—known as central sensitization—is one reason some patients continue experiencing chronic pelvic pain in females even after treatment.
Another major factor discussed in this episode is the role of laparoscopy for endometriosis pain.
Laparoscopy is a minimally invasive surgical procedure that allows surgeons to directly visualize and remove endometriosis lesions. While imaging technologies like ultrasound and MRI have improved dramatically, laparoscopy remains the most reliable method for confirming diagnosis.
However, the quality of the surgery matters.
Excision surgery performed by a highly trained endometriosis specialist can remove disease more effectively and reduce recurrence risk. In contrast, less specialized procedures may leave behind microscopic disease that continues to trigger inflammation and pain.
The experts in this episode also emphasize that endometriosis often coexists with other pelvic conditions, including:
- Adenomyosis
- Pelvic floor dysfunction
- Irritable bowel syndrome
- Bladder pain syndrome
When these conditions overlap, a single treatment approach may not be enough to achieve lasting endometriosis relief of pain.
Instead, patients often benefit from a multidisciplinary strategy that may include:
- Surgical management
- Pelvic floor physical therapy
- Anti-inflammatory nutrition strategies
- Nervous system regulation approaches
- Hormonal therapies when appropriate
This integrated approach recognizes that chronic pelvic pain in females is rarely caused by one single factor.
The episode also explores why endometriosis is still frequently misdiagnosed. Many women are told their symptoms are normal or attributed to other conditions such as IBS. On average, diagnosis can take years, leaving patients to navigate debilitating pain without adequate support.
By understanding the biological mechanisms behind pain—and the evolving approaches to treatment—women can better advocate for their health and access care that addresses the full picture.
Ready to Stop Guessing With Your Endometriosis Symptoms?
If you’re living with endometriosis, you’ve probably been told your pain is “just bad periods,” that birth control is the only option, or that surgery is the only real solution.
But endometriosis is not just a reproductive condition.
It involves inflammation, hormones, immune signaling, the gut, and the nervous system.
When only one piece is addressed, symptoms often persist.
That’s why I created The Endometriosis Reset — a step-by-step program that walks you through the same frameworks and strategies I use with my patients to help calm pain and support the body from multiple angles.
Inside the program you’ll learn:
- The 5 biological drivers of endometriosis symptoms
- How to identify what may be fueling your specific pain patterns
- Nutrition and lifestyle strategies that reduce inflammatory signaling
- Tools to support hormone metabolism, gut health, and nervous system balance
More than 2,000 women joined the waitlist asking for this program, and enrollment is now open.
For a limited time, you’ll also get:
✔ Early bird pricing
✔ Special bonuses
✔ Access to bi-weekly group calls with Dr. Brighten
These bonuses are available for the first 500 women who enroll.
If you’re ready to stop guessing and start supporting your body with a clear plan designed for endometriosis, this is your invitation to join us.
Meet the Doctors in This Episode
Dr. Jolene Brighten
Dr. Jolene Brighten is a board-certified naturopathic endocrinologist, clinical sexologist, and certified menopause specialist. She is the founder of Dr. Brighten Essentials and host of The Dr. Brighten Show podcast. Dr. Brighten is the bestselling author of Beyond the Pill and Is This Normal? and is internationally recognized for her work in women’s hormone health, autoimmune disease, and endometriosis advocacy.
Dr. Ana Sierra
Dr. Ana Sierra is an endometriosis excision surgeon specializing in advanced laparoscopic treatment of complex endometriosis. She has extensive training in neuropelviology and pelvic pain, which informs her multidisciplinary approach to treating endometriosis and related pain conditions.
Dr. Victoria Vargas
Dr. Victoria Vargas is a fellowship-trained minimally invasive gynecologic surgeon specializing in advanced laparoscopic surgery for endometriosis and complex pelvic disorders. She practices in Washington, D.C., where she treats patients with severe endometriosis, pelvic pain conditions, and complex gynecologic surgical needs.
Dr. Shanti Mohling
Dr. Shanti Mohling is a board-certified obstetrician-gynecologist and internationally recognized endometriosis excision surgeon. She specializes in minimally invasive surgery for endometriosis, pelvic pain disorders, and complex gynecologic conditions.
Dr. Cindy Mosbrucker
Dr. Cindy Moss Bricker is a fellowship-trained gynecologic surgeon specializing in excision surgery for endometriosis and complex pelvic pain disorders. She practices in Washington State and is known for her work in advanced laparoscopic surgery and multidisciplinary endometriosis care.
This Episode Is Brought to You By
Dr. Brighten Essentials – NAC
Dr. Brighten’s N-Acetyl Cysteine (NAC) is a high-quality formula designed to support glutathione production — your body’s master antioxidant. It helps promote healthy detoxification, immune resilience, respiratory health, and balanced inflammation.
Support your cells from the inside out.
Exclusive for podcast listeners: Use code POD15 at checkout for 15% off your order.
EndoGlobal Group
At EndoGlobal Group, a network of world-class endometriosis specialists comes together to provide comprehensive, multidisciplinary care for patients with complex endometriosis—offering advanced diagnostic mapping, complete excision surgery, and holistic support.
Click here to learn more and schedule a free consultation.
LUMEBOX
Ready to take your skincare results to the next level—right from home? 💡 LUME Box delivers professional-grade LED light therapy in a sleek, easy-to-use device that targets fine lines, pigmentation, and dullness at the cellular level. Just minutes a day can help boost collagen, calm inflammation, and reveal that lit-from-within glow. It’s the same science trusted in top dermatology clinics, now in your hands.
Shop now → https://drbrighten.com/lumebox use code drbrighten for our exclusive community discount on your purchase.
Related Links
What Is Endometriosis? 4 Surgeons Explain the Symptoms, Misdiagnosis, and Whole-Body Impact Four top surgeons reveal why endometriosis is so often missed—and how it affects far more than your reproductive organs.
Endometriosis Symptoms vs Normal Period Pain with Dr. Patrick Yeung If you’ve ever wondered whether your period pain is normal, this expert explains the red flags doctors too often miss.
The Hidden Link Between Your Gut Issues and Endometriosis | Dr. Jill Ingenito Bloating, IBS, constipation—this doctor explains why gut symptoms may actually be endometriosis.
Endometriosis Diet That Stopped 20 Years of Pain | Khush Sra After two decades of severe endometriosis pain, these nutrition strategies changed everything.
Doctor Reacts to Lili Reinhart and Breaks the Endometriosis Diagnosis Myth | Dr. Jolene Brighten Dr. Jolene Brighten reacts to Lili Reinhart’s story and exposes the biggest myth about endometriosis diagnosis.
Endometriosis, HRT, and Menopause: Expert Answers on Surgery, IVF & What Really Helps| Dr. Melissa McHale What happens to endometriosis in perimenopause and menopause—and what treatments actually help.
Endometriosis Awareness Month: Special Episode Clips The most eye-opening moments from the Endometriosis Expert Series, all in one powerful episode.
ADHD Endometriosis Connection: What You Should Know If You’re Diagnosed with ADHD Why ADHD and endometriosis show up together more often than you might expect—and what that means for your health.
How to Tell If You Have Endometriosis. Painful Menstruation, Symptoms, and Treatment | Dr. Ramiro Cabrera An endometriosis specialist explains the symptoms that signal it’s more than just a painful period.
Pain During Sex, Causes, Symptoms & When to See a Doctor | Dr. Ana Sierra Painful sex isn’t normal—here’s what your body may be trying to tell you.
The Hidden Connection Between Estrogen and Histamine: Why Your Hormones Cause Inflammation If your allergies, headaches, or rashes worsen around your cycle, estrogen and histamine may be the reason.
What Is Adenomyosis & How Is it Treated Heavy periods and pelvic pain could be adenomyosis—here’s how it’s diagnosed and treated.
Endometriosis Treatment: A Doctor’s Guide to Surgery Prep and Recovery What every patient should know before endometriosis surgery—and how to recover the right way.
19 Ways to Find Endometriosis Relief Naturally Science-backed strategies to calm inflammation, reduce pain, and support your body with endometriosis.
Best Supplements for Endometriosis (Evidence-Based Guide) The supplements with the strongest research for reducing inflammation and supporting endometriosis symptoms.
FAQ: Endometriosis Pain, Laparoscopy, and Chronic Pelvic Pain in Females
Endometriosis pain is driven by a combination of factors including inflammation, hormonal signaling, immune system activation, and nerve involvement. Lesions can release inflammatory compounds that stimulate surrounding nerves, contributing to severe pelvic pain.
Laparoscopy can significantly reduce pain when performed by a skilled surgeon who removes endometriosis lesions through excision. However, because endometriosis is a chronic inflammatory condition, some patients may require additional treatments to manage symptoms long term.
Over time, repeated pain signals can lead to changes in the nervous system. This process, known as central sensitization, can make the body more sensitive to pain signals and contribute to chronic pelvic pain even after initial triggers are addressed.
Many endometriosis lesions are small or located in areas that imaging technologies cannot easily detect. This means scans may appear normal even when significant disease is present.
Effective treatment often requires a combination of approaches, including surgery, pelvic floor therapy, anti-inflammatory lifestyle strategies, and hormonal management depending on the individual patient’s needs.
No. Endometriosis can affect multiple body systems, including the digestive system, bladder, nervous system, and immune system. That’s why many experts now consider it a whole-body inflammatory condition rather than solely a gynecologic disorder.
If you or someone you know is struggling with endometriosis pain or chronic pelvic pain in females, this episode offers insight into why these symptoms occur and how treatment approaches are evolving. By bringing together expert perspectives, the goal is to empower women with information that helps them better understand their bodies and advocate for the care they deserve.
Transcript
Dr. Brighten: [00:00:00] If pain were taken seriously in women, endometriosis wouldn't take a decade to diagnose. Their pain is real because the experience of the pain is going to be real for them.
Dr. Shanti Mulling: There's no evidence that a birth control pill decreases a lesion, prevents recurrence, or in any way treats endometriosis.
Dr. Victoria Vargas: There's this misconception that if you remove the ovaries that you're curing, endometriosis studies have shown that when you have your ovaries removed at a young age, that you die at a younger age from all cause mortality, including heart disease, dementia.
Dr. Cindy Mosbreer: If you go to a gynecologist and they don't want to listen to you about your pain, they're not gonna do you right. If they operate on you, you don't want to see that person. You just need a different doctor.
Dr. Brighten: What is the deadliest part of living with endometriosis?
Dr. Ana Sierra: Not finding a proper surgeon to do your surgery?
Endometriosis is a high morbid disease because the way that it affects your life, it's not so many cases that you know of that they have mortality, but if you [00:01:00] are a counter, a non-skilled surgeon, it can be fatal for you.
Dr. Brighten: You were telling a story about a patient who recently died because their, the surgeons were completely out of their depth.
Dr. Ana Sierra: Yes. And they had, uh, a iliac vein. Uh, it's a iliac vein, has a lot of blood flow that comes from the leg up to their heart, and they weren't able to fix it so the patient dies. So I think it's really important that not only you find a very good surgeon that cares for you, that you find a skilled surgeon that does the thing that she sells, that he is telling everybody that does.
Dr. Victoria Vargas: I think you are much more likely to have your ovaries removed at a young age with endometriosis. And studies have shown that when you have your ovaries removed at a young age, that you die at a younger age from all cause mortality, including heart disease, dementia. Um, the ovaries have a very important function, but there's this misconception that if you remove the ovaries that you're curing endometriosis.
Dr. Cindy Mosbreer: Women after [00:02:00] IVF develop these nodules where they didn't have them before and then after IVF, they, their endometriomas grow, their, their nodules that are obstructing the ureters grow and nobody wants to do anything about it.
Dr. Brighten: Mm-hmm. So here's the thing. If pain were taken seriously in women, endometriosis wouldn't take a decade to diagnose.
I'm Dr. Jolene Brighton. I'm the host of the Dr. Brighton Show. I'm a board certified naturopathic endocrinologist and a patient with endometriosis and adenomyosis. And I am joined by some of the most brilliant endometriosis specialist that you can find in the world. And I'm gonna have them introduce themselves now.
So, Cindy, would you mind introducing yourself?
Dr. Cindy Mosbreer: Hi, I am Cindy Moss Brier from Gig Harbor, Washington, and I've been doing endometriosis as well as, uh, urogynecology Endo for the last 20 years, Urogyn for the last 30 years.
Dr. Shanti Mulling: Hi, I am Shanti Mulling. I am living and working in Portland, Oregon [00:03:00] at Northwest Endometriosis.
Pelvic surgery. Um, currently my specialty is endometriosis and pelvic pain.
Dr. Victoria Vargas: I'm Victoria Vargas. I'm a minimally invasive GYN surgeon with a specialty in endometriosis surgery based in Washington DC, and my practice is called Washington Endometriosis and Complex Surgery.
Dr. Ana Sierra: Hi, I am Dr. Anna Sarah. I am an exec surgeon with neurobiology training and I work here in Mexico City.
Dr. Brighten: And what is neurobiology for everybody? Listening.
Dr. Ana Sierra: Neurobiology is an answer for a lot of people that doesn't know about the nerves in the pelvis. We have the same amount of connection in the pelvis that we have in our brain, so I think it's a wonderful thing. Um, the quote that got me into this was pain is not a disease.
Pain is information that travels through the nerve. So I think that is one of the best answers that get into me when I started studying this, because if [00:04:00] we stop treating pain as the enemy and we see it as clues that help us to resolve the diagnosis, it's so much better than just numbing the pain and giving them opioids.
Dr. Brighten: Why is it? This current year of 2026, as we speak, women are still treated like they're being dramatic when they go to their doctors about pain.
Dr. Victoria Vargas: I think there's just such a stigma about female reproduction. You know, it's, it even impacts our education in medical school about women's reproductive health.
There's just such a lack of knowledge about what's normal when it comes to menstrual periods. Um, many doctors don't even know that you make a cyst of ovulation. And I think there's just a lack of knowledge. People think it's normal to have pain with your period. And I think, unfortunately, I think this is all based in misogyny in our medical field.
Dr. Brighten: So, Ana, I wanna ask you what happens when women's pain is dismissed early in life?
Dr. Ana Sierra: It delays the treatment and it delays the diagnosis. Even if it's [00:05:00] endometriosis or it not endometriosis, if you dismiss the pain and tell them that it's normal, the patient is going to have a lot of consequences after this.
We've talked about the way that having chronic pelvic ca pain changes your brain.
Dr. Brighten: Mm-hmm.
Dr. Ana Sierra: So I think it's really important to address the US early so you won't have a life of pain.
Dr. Brighten: Can you say more about how it changes your brain? Because I think a lot of times women go to the doctor and they hear this pain is normal.
So they try to suck it up. They try to power through it. What is actually happening to the brain that patients should be aware of, but that for our clinicians listening, they should have been taught in medical school.
Dr. Ana Sierra: MRIs of the brain of people with chronic pelvic pain or just not, or chronic pain changes.
Patients with fibromyalgia. Patients with endometriosis have changes in the prefrontal prefrontal cortex. In the thalamus. In the insula, it's different. The, it rewires them in order to feel, uh, pain more easily. [00:06:00] We are known to have neuroplasticity, and if you repeat something, you're gonna be very good at, if you're learning, I don't know, the multiplication tables or something that you go two by two is four to it.
Every time you say it, you're gonna be either even better to recollect the information. So for a patient that has. Endometriosis and this immune cells are secreting neurological growth factor that makes neurons, uh, irrigate or innervate directly. The lack of endometriosis, this neuron is having the information of inflammation every day, all days.
So for them it is really easily to recollect the information of pain in the asali and going into the brain and to stimulate the centers of nerves In one point, you don't even need the stimulus to feel the pain. So that's the point that we don't want them to get because if the patients get to that point, it's even harder to treat because you need to rewire [00:07:00] again.
Mm-hmm. The brain.
Dr. Brighten: Does that give clinicians permission to say, your pain is all in your head
Dr. Ana Sierra: because it's not in the head, it's real.
Dr. Shanti Mulling: It's gonna be in your
Dr. Ana Sierra: head. And the experience is the same for them. The thing is that they have to understand that for them, they are feeling the same thing that they were feeling even before the excision surgery, but the wires have been so deeply patented that they cannot change them by themselves and they are not crazy.
Dr. Brighten: Ashanti said something very controversial in our first episode, which you all find linked. I would definitely recommend going back and listening to that. And you said against acog, you would recommend in some teenage patients to have excision surgery.
Dr. Shanti Mulling: A absolutely, and I've, I've found stage three plus disease in teenagers that would've gone unrecognized.
And because that by nature is deeply infiltrative disease, it will worsen with time.
Dr. Ana Sierra: Could you explain what is, uh. Uh,
Dr. Shanti Mulling: stage three. Excellent. Yeah. So, um, patients with [00:08:00] endometrioma with, uh, disease, approaching the rectum, that that ultimately could become a disease that you have to do a bowel resection or in teenagers.
In teenagers, right, that I've taken care of removing the disease very carefully and somewhat conservatively compared to an older person. It makes a very bright impact on their lives. And so I, I realize it's really controversial, one to say, don't necessarily jump to birth control pills, combination especially, and two.
To say, go ahead and excise disease in these teenagers,
Dr. Brighten: and that's where I think ACOG has been very problematic in endometriosis care.
Dr. Cindy Mosbreer: Well, and worse than giving people birth control without a diagnosis, ACOG says it's fine to give them Lupron without a diagnosis.
Dr. Brighten: You go off. What is Lupron? Tell the people.
Dr. Cindy Mosbreer: One of the biggest problems with it is that once you get that injection, you cannot get rid of it until it wears off. It is what's called A GRH [00:09:00] Agonist, and GNRH is gonadotropin releasing hormone, and it is made in the hypothalamus. The hypothalamus is the part of the brain that is just above the pituitary gland.
GNRH goes down to the pituitary and stimulates the pituitary to make follicle stimulating hormone. Follicle stimulating hormone has the most clever name in the world because what does it do? It stimulates the ovaries to make follicles and to grow. A follicle is a cyst that contains an egg that eventually will ovulate.
And so GNRH is released in pulsatile manner, and the agonists give, basically, they act like GNH, but they take away that pulsed, uh, nature of it to, to give a constant dose of GNH, which then suppresses FSH, which then does not allow the ovaries to make the [00:10:00] follicle, and it decreases the amount of hormone production by the ovary.
So essentially they induce menopause. Nowadays we have, uh, or Alisa, which is a g Gnh antagonist, but it works the same way. Mm-hmm. Does exactly the same thing. The biggest study back in the, uh, eighties of Gnh agonists for endometriosis actually didn't even use Lupron. It used three other GNH agonists that were available in, in Europe.
There were multiple. Studies that actually got published. There were hundreds of studies that never got published, and I know this because Dr. Redwine was the expert witness for a class action suit of women against the was originally tap, and then I think it was by by, was it Bayer? Or there was another pharmaceutical company that bought the patent for Lupron.
He was the expert witness and he [00:11:00] got access to all of the data that they suppressed because they didn't want it to come out. How damaging Lupron was to the ovaries.
Dr. Brighten: What information was the pharmaceutical industry suppressing to get women to buy into this drug?
Dr. Cindy Mosbreer: The biggest thing that sticks out to me is that the peak estradiol levels never recovered.
So at ovulation, estradiol levels peak between three and 400 nanograms per deciliter or whatever the stupid units are. They're ridiculous.
Dr. Brighten: So people know we're really good at reading the numbers, but you get far enough in practice, you're not looking at units anymore.
Dr. Cindy Mosbreer: Yeah. So peak estradiol at ovulation is in most women in their twenties and early thirties, is somewhere between three and 400 after Lupron.
Even if it was only given for six months, it never got that high. And in some it was only like between 102 hundred and a hundred is where [00:12:00] we want postmenopausal women to be so that they have protection for their bones and their brain, the vagina and their bladder, and everything else that we wanna protect.
It's not enough for a 20-year-old. It's not enough for a 30-year-old. It's probably not barely enough for a 40-year-old.
Dr. Brighten: Yeah.
Dr. Cindy Mosbreer: And so, and Orissa was the same way. There. There was like three or four or five times more studies that were suppressed and never got out, never were published than the studies that were actually published.
And even the studies that were published show a very low response for deeply infiltrating disease. So the best response with Lupron was not surprisingly for the symptom of dysmenorrhea, what is dysmenorrhea? It's cramps through, through period. What does Lupron do? It takes away your period. Big whooping deal.
Dyspareunia, which is pain. Pain with sex painful bowel [00:13:00] movements, other markers of more deeply infiltrating disease never changed with these drugs yet they were marketed as, oh, give all your patients with endo these and they'll make 'em better. I think that I have prescribed Lupron probably maybe once or twice in the last 20 years, and it's because somebody actually came in and said, I can't have surgery until November.
Please. The birth control isn't working. The progestin isn't working. I did fine on it three years ago. Will you please put me on this so that I can hang on until and get through all everything I have to in life? Until then,
Dr. Brighten: so everyone listening, episode four, we're gonna go deeper into hormones, but what I wanna underline here is that you pointed out.
Postmenopausal women when we're doing hormone replacement therapy, specifically estrogen hormone therapy, we wanna see serum levels at a hundred. That is to maintain bone density when [00:14:00] you're in your twenties, when you are a teenager. We need to be building bone density, and that is why we need those higher estrogen levels.
And so I think that really feeds into what Shanti was talking about, about how we're treating teenagers. And I think it is a slippery slope of treating teenagers as if they're the same as a 30-year-old, as if they're the same as a 40-year-old. And like we see so much of women's medicine is like, you have a period, y'all are the same.
Like you don't have a period. Why are you worrying about anything now? And I think that there's just a lot of dismissal. When I wanna shift the conversation though is asking, because we're so often told. This is just a pelvic disease. Where are some of the craziest places you have seen colleagues or yourself personally find endometriosis in women?
Dr. Victoria Vargas: I'll say the inguinal canal.
Dr. Brighten: With the inguinal canal for women who don't know.
Dr. Victoria Vargas: So it's, it's just growing and I've, you know, I see it there. And in the mons I've seen really large lesions on the mons, and I feel like no one really talks about these types of, and do you think that retrograde menstruation could cause that?
[00:15:00] No.
Dr. Brighten: Not at all. Me neither. Y'all need to get that joke in episode one.
Dr. Ana Sierra: For me, it was a spleen. The spleen. When, when I was training into end the jersey surgery, I remembered my teacher telling me, you're never gonna find endo in the spleen because it's immune tissue and it will defend itself out of, uh, the disease.
And I've, uh, performed to splenectomies. That's the same thing in English. Yes. Because of ome disease. So, yeah. Well, me and my team, of course, but yes. So yeah.
Dr. Brighten: How about you, Cindy?
Dr. Cindy Mosbreer: Uh, I had a patient once who would bleed out of her ear every time she had her patient.
Dr. Brighten: Period. Oh my God. We should be like, you know, playing a game here.
I think you just won eating out ear.
Dr. Cindy Mosbreer: Wow.
Dr. Ana Sierra: But there have been reports on the eye, on the nose. Yeah. The larynx. There
Dr. Brighten: was just the wrist. But
Dr. Shanti Mulling: we, we don't all get to see that.
Dr. Brighten: Yeah. You know. Well, I understand. I see a
Dr. Shanti Mulling: lot in the belly button.
Dr. Brighten: As an endometriosis patient, every time you have a twinge or an ache or a pain somewhere, you're like, [00:16:00] could it be endo?
It's, it's a real theory. Live with, even after excision surgery of like. Could it show up somewhere next?
Dr. Shanti Mulling: I found it on the surface of the kidney that way. So that's one. I also have a patient coming up in a couple of weeks who does cough blood with her period and has a pulmonary lesion. And by the way, for our listeners, if you have that symptom, you definitely need a proper evaluation.
And most of the time to actually see a lesion like that on CT or MRI, it's really best if you are on your period when you get those imaging studies done to be able to visualize that in the, in the pulmonary. Uh, region.
Dr. Brighten: Does it need to be like day one, two of your periods? Like is there a window?
Dr. Shanti Mulling: It's during the whole cycle of when you're bleeding me menstrually anyway, that you, uh, are gonna be able to highlight it, um, on the pulmonary lesions.
Dr. Brighten: How common is thoracic endometriosis? Is it more common than women might be aware of?
Dr. Shanti Mulling: I think it's probably more common than [00:17:00] even practitioners are aware of, but diaphragmatic disease is, is 10%, 90% of that is gonna be on the right side. Um, but I, I suspect that it's higher than that. You know, the, the, if you think about it, nausea, reflux symptoms, chest pain, rib pain, um, coughing, coughing blood is an extreme case, but just coughing and irritation and shortness of breath during the period might be symptoms.
And so. The, some of the patients I've diagnosed have had 1, 2, 3 prior laparoscopies where no one saw the disease. And I can think of patients where I, I, my first glance up into the upper abdomen, you don't see the disease, but when you go and look, you find the disease. It's easy to find if you're comfortable just taking a look.
But if you don't really feel comfortable just even just pushing on the liver or lifting, elevating it to look underneath it, you won't find the disease that exists. So I suspect it's [00:18:00] higher than 10%.
Dr. Cindy Mosbreer: A lot of times it's at the very back of the liver and the very most posterior aspect to the diaphragm and the liver is domed.
And so it's challenging to get the liver pushed down enough.
Dr. Shanti Mulling: Once you're close and you're one, once you're more central, close to that central tendon, you also are in a greater danger zone of, of injuring the phrenic nerve. So it's, it's definitely. Not the thing that everyone is gonna be attacking as an endos surgeon.
Dr. Brighten: We've talked about you, you saying chest pain often gets chalked up to just being anxiety in women. At what point of this, like ignoring these symptoms or blaming these symptoms on something like anxiety, does it become negligent?
Dr. Shanti Mulling: One of the dangers, uh, would be providers like emergency providers, pulmonary doctors, cardiothoracic surgeons who will treat [00:19:00] pneumothorax, uh, in a, in a typical way that you might treat someone who didn't have endometriosis.
And so women who present with pneumothorax a collapsed lung cavity, which. W can happen in the presence of endometriosis on the diaphragm or, or in the pleura of the lung. And they treat it, um, with a procedure to seal the, the pulmonary cavity. And then you can never go back in and remove the disease. So they won't have a recurrent pneumothorax necessarily, or they will have, um, but they'll continue to have pain.
And, and I've, I've read reports in the cardiothoracic literature of how fabulous this is, how we were succeeded for six months. We, we, we did a ple Desis by, you know, Taal in the lung. We sealed off the cavity and we gave her Lupron or, or Alyssa for six months and she hasn't had a recurrence. So great. So then she's gonna go off the Alisa, you know, so, [00:20:00] so you can't stay on Arissa for life.
So that's wonderful. They've treated her for six months, but she's, she'll still have the symptoms when she comes off the Alisa, and she'll still have pain even if she doesn't have a pneumothorax.
Dr. Brighten: Pneumothorax, collapsed lung. This is happening in emergency situation. What could be done better?
Dr. Shanti Mulling: It could be recognized that a pneumothorax has a very high likelihood in a woman of being related to endometriosis.
And an endometriosis could be called in addition to perhaps a cardiothoracic surgeon,
Dr. Cindy Mosbreer: especially when it's a recurrent thing and it always happens on their period. There's actually a name for that. It's called Catamenial Pneumothorax.
Dr. Shanti Mulling: Indeed. Yeah.
Dr. Brighten: So the, the thing that clinicians should be doing is bringing in the endo expert with female presents pneumothorax.
It is an endo expert who also is accompanying them in the room to make sure that we know what we're dealing with and that we're not seal off a cavity and making it so that this is, becomes untreatable.
Dr. Shanti Mulling: Exactly.
Dr. Ana Sierra: Refer the patients to the [00:21:00] experts. We have a patient that, um, have fenestrations on the diaphragm and they placed a mesh on top of it.
So removing the disease with the mesh on top of it. Uh, no. Yeah.
Dr. Cindy Mosbreer: Can I, can I just make a comment? Simple things being simple. The vast majority of patients with chest pain, 98% of the time is myofascial pain and comes from a super tight pelvic floor and the spasm on the inside of the pelvis. Extends out to the outside of the pelvis and then it goes up.
It also can go down. These gals get a lot of really tight IT bands. They get pain in their hips, they get pain in, typically, it's whichever side of that. The pelvic floor is more spastic in. So I don't want everybody who is listening to think, oh my God, I have pain in my chest. I [00:22:00] must have thoracic endo.
The vast majority of women with endo who have upper abdominal and chest pain, it is myofascial in the PTs, can help you with it.
Dr. Brighten: That's great. And but I think also to Shante's point, if you're gonna have laparoscopy, they should at least be checking the diaphragm during that. And so I think that's a good take home for patients is like.
It doesn't mean that this is thoracic endo. However, if you are going to have the surgery, we wanna ask that the surgeon's gonna check that. And I think that's a good question. We're gonna have more questions that people should ask their surgeons, but is also, you know, I think a really good one is like, do you check the diaphragm during surgery?
I am curious what symptoms should never be brushed off without anatomical investigation.
Dr. Shanti Mulling: I like all symptoms.
Dr. Brighten: All symptoms. Okay.
Dr. Shanti Mulling: I, I mean, so I think we blow off things like, uh, as, as widespread practitioners, we, we, we [00:23:00] don't pay too much attention to fatigue, to nausea, to reflux, uh, to chest pain. We just assume it's anxiety.
However, sometimes that nausea can, I, I've had patients where you'd remove their, their diaphragmatic disease and their daily chronic nausea and vomiting goes away.
Dr. Victoria Vargas: Mm-hmm.
Dr. Shanti Mulling: It's like, it's like a miracle. And so if we are blowing that off and just saying, oh, well you must be taking too much nonsteroidal NSAIDs and ibuprofen and, and so that's why you have gastritis.
We might be missing something. Mm-hmm. And maybe 10% of the time we are,
Dr. Brighten: I wanna discuss pain management further, but first I wanna hear it from you. What is the most unhinged endometriosis intervention a patient is brought to you that you then discovered actually worked?
Dr. Victoria Vargas: I feel like a lot of my patients on GLP one have told me that their inflammation and pain has improved while they've been on that medication.
Dr. Ana Sierra: I really have learned a [00:24:00] lot from our, uh, physical therapists. And one of them tell me that, uh, there's an association between the dysfunction on the pelvic floor and the temporal mandibular jaw.
Dr. Brighten: Oh yeah.
Dr. Ana Sierra: So there's some form of treatment that can be done on the same, because most of this patients have an alteration in the temporal mandibular jawline.
Dr. Brighten: Yeah. There's been, um, so doing a OID release, which I'm not gonna do it 'cause I have lipstick on, but if you're watching you to get thumb in your mouth and actually releasing the, the jaw, some women will say like, yeah, my like. A pain with sex. It was like easier to have intercourse. Like there's been some really interesting things that patients will report when they get that.
And um, the first time I ever heard it was Botox. Someone got Botox for their TMJ. Mm-hmm. And then they're like, oh, everything is feeling better downstairs. And I'm like, say more, say more about this. Uh, Cindy, did you have something you wanna add?
Dr. Cindy Mosbreer: I mean, it's not really unhinged, but I mean, we share a lot of patients with naturopaths [00:25:00] and, um, I have a lot of gals that are on, uh, NAC and glycine, uh, which are co-factors in the production of glutathione, right?
Mm-hmm. Yes. And glutathione is like one of the biggest free radical scavengers in the body. And, uh, anti-inflammatory diets. I used to be so skeptical and now I'm like, you know, doing anti-inflammatory diet.
Dr. Shanti Mulling: I was gonna bring up NAC as well. We have data, we actually have research data that shows. An endometrioma can shrink a little bit by taking daily an acetylcysteine and about as much as it shrinks by taking a birth control pill.
Dr. Brighten: Mm-hmm. Yeah. And the what's interesting, the studies are sometimes using 600 milligrams, but it seems to see be, the sweet dose is like 1200 to 1800 milligrams a day. And often people will say, well, oh, they only have the patients take it for three months. So you take it for three months and then you don't need it.
And I'm like, as someone who's been on n [00:26:00] acetylcysteine for like. Probably 20 years. It's like one of the things that when I learned about it, it's gotta be like one of my favorites, you know, I'll share, one of the unhinged things that I found I wasn't expecting is the vibration plates that went viral on social media.
I got them like, I got it like years in advance. 'cause I was like, I wanna challenge my balance when I'm working out and I'm doing weights and it's great for lymphatic. And I started doing stretches on it. And when I went back to my pelvic pt, Deanna, who, you know, she was like, what did you do different from last week and this week?
Because your pelvic floor is completely different. And I'm like, I stood on a vibration plate. Leaned forward on a bar and like shaked out my, I shook out my hips and did all of these stretches on it, and it completely, she's like, you've like released so many trigger points. So that's my unhinged share.
What I wanna ask you, Vicki, though, is why don't NSAIDs and opioids address endometriosis pain adequately?
Dr. Victoria Vargas: I mean, because it's, they're not really targeting the source of the pain, to be honest. I feel like NSAIDs can be a little [00:27:00] bit helpful because they impact inflammation. But especially if you have like deep infiltrating nodules and Anna.
Was speaking about this, they have their own like nerve endings that are, you know, you're not gonna improve pain from something infiltrating into your rectum with any medication. I mean that it's gonna take surgery to make you feel better.
Dr. Brighten: Let's talk a little bit about how these lesions are different.
'cause we, we talked about it a bit in episode one, but you just said they, they make their own nerve endings. Yeah. What about these lesions make them challenging to treat?
Dr. Victoria Vargas: Because they infiltrate tricky areas like the rectum, the cecum, the, the small intestine. They infiltrate nerves. Um, the bladder, the ureters.
I mean these are very delicate areas with surrounding structures that, you know, you really have to have a high level of expertise to treat them. And medical management, unless you're completely asymptomatic from them, medical management isn't gonna do anything if you're having pain or symptoms or even infertility.[00:28:00]
It's surgery's really the only answer for these types of lesions.
Dr. Ana Sierra: Is there anything you'd add to that, Anna? No, um, uh, I just, I'm thinking about, um, whenever you have a patient in pain, I will think about the pain as an experience. And if you think about patients in pain, some of them will have a different, the different, the experience would be different.
If they're with their family that, and were alone, then when their work life, uh, balance is different or if they have some kind of support, the pain they feel is different even though the signal is the same. So pain is not only signals. And there's a difference there.
Dr. Brighten: And speaking of difference, I wanna ask you, what is the difference between inflammatory pain versus residual nerve pain, and why does this difference matter?
Dr. Ana Sierra: Uh, it, it's difference in the origin, but for the patient is going to be the same experience.
Dr. Brighten: Mm.
Dr. Ana Sierra: So I think that we, what we should address as clinicians is the [00:29:00] difference between visceral nerve or, or visceral soma, uh, visual pain and somatic pain because as Vicky was saying, uh, visceral pain is a pain that your patient cannot tell you.
Where is it? It's endometriosis pain. Everything hurts. And it's associated with neuro vegetative symptoms. Like when I have the pain, I'm, I, I, I'm pale. Um, my hairs are like standing
Dr. Brighten: out. Standing out. Yeah,
Dr. Ana Sierra: I have nausea. I want to vomit. That's visceral pain. And, uh, somatic pain, they're gonna show you when one finger here, it hurts here.
So we're talking about different types of transmitting the pain and a different type of source. If you start by this, you will start defining the e theology of the pain, and maybe you're onto something into helping them.
Dr. Brighten: We talked a lot at the beginning about what. Long-term pain can do in changing the nervous system, in shaping the brain in shaping your future experience.
And we promised we'd come back to some solutions around this. [00:30:00] What are things that can actually help with pain?
Dr. Ana Sierra: Neuroplasticity can go both ways. So it can go on the way that you have shape or life has shaped your brain into being very good at feeling pain. But they can also be very good at remembering how your pelvic floor functions.
So we have found that, uh, pelvic floor therapy is really helpful in order for them to feel different experiences, especially with patients with endometriosis that they no longer recognize, do I want to pee or does I, do I have pain? Do I, because you know, uh, the muscle activity is like the window. Mm-hmm.
It's, it's a window to the way that. Our patients deal with the world. So if you find a contractor at PAL with it is because they are hiding or they're protecting themselves against their pain. So if we start addressing this and start teaching them our, one of the things that, doing a scan and seeing what is this?
This is pain in my bladder. This is wanting me to be, [00:31:00] to, again, starting to recognize the real signals on your pelvic floor. It's going to help you. Lot
Dr. Brighten: physical therapy.
Dr. Ana Sierra: Yes.
Dr. Brighten: Body scan.
Dr. Ana Sierra: Yes.
Dr. Brighten: All right. Is there any other lifestyle therapy, Cindy?
Dr. Ana Sierra: Yes.
Dr. Brighten: Cindy wants to,
Dr. Cindy Mosbreer: well, there was a, there was a study, uh, about 10 years ago where they had patients with endometriosis of all stages, and they measured markers of central sensitization pre-op.
And what they did was they did. A pressure test. So they took, took a something and pushed on forearms and they measured how much pressure did it take before the perception was pain instead of pressure, how much force did it take before the patient perceived it as pain? Instead of pressure. Then they operated, they, they, uh, did good excision surgery, and then at six months post-op and 12 months post-op, they reassessed these [00:32:00] markers of central sensitization and guess what?
They got better.
Dr. Brighten: Mm-hmm.
Dr. Cindy Mosbreer: And so every primary pain stimulus that you can remove helps to reverse central sensitization,
Dr. Victoria Vargas: and that's why it's so important, I don't know, to to treat the entire disease, the overlapping conditions, and also the endometriosis, and not deny patient surgery when they need it, because it may be.
One way to remove a pain,
Dr. Cindy Mosbreer: but if they also have hip impingement, you know, yeah. That needs to be dealt with. If they have herniated discs, if they have, uh, you know, if they have thoracic outlet syndromes, if they have all these other things that you can get, you know that some of them come from a tight pelvic floor and then everything gets twisted and then your whole axial skeleton doesn't work.
Right.
Dr. Brighten: I wanna get into some more specifics about pain, but first I wanna play two truths and a lie with Anna. Okay. So I'm gonna make three statements and you are gonna let the listeners know, which [00:33:00] is a lie. So the first one, you can walk but still have severe nerve involvement. Two. Botox can be used to treat nerve pain.
And three, birth control is the best treatment option to stop the progression of endometriosis, which is the lie.
Dr. Ana Sierra: The last one is the lie.
Dr. Brighten: So why does this lie persist?
Dr. Ana Sierra: Let's, let's think about each one of the sentences that you said, because I think all of them are really important. First of all. Yes, you can walk and still have nerve involvement because there are a lot of nerves.
And sometimes my patients tell me, oh, I have sciatic pain, so I should have endometriosis in the sciatic nerve. No, that's not it. I mean, first of all, the sciatic is not only pain on the backside of your leg, it goes all the way into your feet. If it's only on the backside of your leg, it's probably a fem, a posterior femoral ous nerve or another cause.
And there are a lot of causes of, uh, satic nerve impingement, for example. Now that running, its so hip [00:34:00] and fashionable. Uh, I have a lot of pain, uh, patients that have the per pyramid. No, his muscle pinching the sciatic nerve because that's the way that it exodus. So. It's not always about pain on the legs.
You, I think the most common, uh, nerve entrapments by endometriosis are the autonomic systems because you're gonna find more patient that have pelvic floor dysfunction, that have problems emptying their bladder, uh, dysfunction in the sexual, having sexual intercourse or emptying, uh, their. Rectum. All of those are nerve compressions because of the autonomic system are so much more common than somatic.
So I will go first with that one. Second, uh, Botox can be used to treat nerve pain. It is because it can block the signal and it can help them as a neuromodulator and in order for them to help ease the pain and also forget the pain, and it helps to [00:35:00] this neuromodulation and this, um. Changing the way that the patient feels the nerve.
So that'll be the second one.
Dr. Brighten: Wait, I am gonna ask you more about Botox. Okay. Is that a standalone treatment or do you use it in conjunction with other therapies?
Dr. Ana Sierra: It depends on the, the cause and it depends on the patient.
Dr. Brighten: Mm-hmm. But would you just tell someone just have Botox for your nerve pain indefinitely?
Dr. Ana Sierra: No. And also I wouldn't have a patient have Botox on the, sometimes they just tap and add Botox where the, whenever there's pain, if you do that, you're not finding the cause of the pain. You're just numbing the pain and the places where it hurts. So you have to find the nerve and then you block that nerve.
Or if you're seeing a muscle, you're gonna try to fix that nerve, that muscle. But you need to know the anatomy of the muscles and the pelvic floor. If you're just. Placing Botox, whatever it hurts you are, you're not gonna have very good results.
Dr. Brighten: Who should you see for this treatment then? Because we don't want the tap and poke.[00:36:00]
Yeah. Who do we want?
Dr. Ana Sierra: Uh, pelvic vein specialist. I would go with that and ask the doctor what technique do they use before they use it on you?
Dr. Brighten: Okay. Now tell us why is it so many doctors? I mean, I have seen very large podcasts have doctors on who say the best way to stop the progression of. Endometriosis is to take the pill.
Why is this wrong?
Dr. Ana Sierra: I think because you are not addressing the inflammatory component, and you should, because endometriosis is so much about the inflammation and, uh, stopping, uh, menstrual cycles does not fix the problem.
Dr. Brighten: Mm-hmm.
Dr. Ana Sierra: So,
Dr. Brighten: so I'm gonna say, I'm sitting here with four of the top female endometriosis experts.
So I just wanna clarify, have there ever been any quality evidence studies showing that birth control slows down the progression of endometriosis?
Dr. Shanti Mulling: Well, yes, but only ovarian disease.
Dr. Brighten: So only endometriomas
Dr. Shanti Mulling: only preventing formation [00:37:00] of recurrent endometriosis of the ovary chocolate cyst endometriomas.
Yeah. And so we have a study showing it will help prevent recurrence to be on a birth control after excision of the endometrioma, but. In the rest of all the literature in, to my knowledge, there's no evidence that a birth control pill decreases a lesion, prevents recurrence, uh, or in any way treats endometriosis.
Dr. Brighten: Well, I just wanna clarify exactly what you just said, is that this study showed excision first, then the birth control pill for only the, the lesion in the ovary. It wasn't
Dr. Shanti Mulling: correct.
Dr. Brighten: No surgery at all
Dr. Shanti Mulling: for an endometrioma.
Dr. Brighten: Mm-hmm.
Dr. Shanti Mulling: Perfect.
Dr. Brighten: Yes. Vicky, what were you gonna
Dr. Victoria Vargas: say? I was just gonna say I, Horace Roman, he did his 10 year follow-up study of patients who had surgery for most of them, had deep infiltrating endometriosis of the bowel, and [00:38:00] he found that the patients who were put on some form of hormonal therapy post-surgery were less likely to need surgery after.
If you're man using it for management of adenomyosis, it may help you from having a hysterectomy.
Dr. Brighten: I'm gonna, I'm gonna challenge this.
Dr. Victoria Vargas: Yeah.
Dr. Brighten: Because I have had endometriosis experts. Yeah. On the podcast. Dr. Patrick Yung has actually done a study showing it is possible to do one in Stu done surgeries, and I'm paraphrasing him, so if I get this wrong, Patrick, I apologize.
But essentially, one of the arguments he made is that the use of hormones afterwards, it's kind of a buffer. So you don't have to do that good of a job of a surgery. So like a surgeon doesn't have to have the aim of, let me try to get everything and clear out all these lesions because they know they have the padding, the fallback, the comfort of I can suppress their hormones afterwards.
So I agree with that. A hundred
Dr. Cindy Mosbreer: ris Ramon is one of the best surgeons in the universe. Yeah. And that is not what, that is not his.
Dr. Brighten: [00:39:00] Yeah.
Dr. Victoria Vargas: What I wanna
Dr. Brighten: say, uh, it may not be his mindset, but what Patrick's argument and others have made is that surgeons will sometimes go into it being like, meh, I don't have to do as good of a job because I can always fall back on birth control.
I'm not saying this individual. I don't know Horace. Yeah.
Dr. Victoria Vargas: Not that you should not have him on your podcast. I'm not pointing fingers. You should invite him.
Dr. Brighten: Sorry, Horace, I don't know.
You,
Dr. Victoria Vargas: you should have him on your podcast. But I, what I wanna say is I could see how that, what I'm saying could be interpreted that way, but that's not how I am intending it at all.
The thing about the reason I trust. Horace Roman study is because he has a YouTube channel and he literally posts his surgeries on there.
Dr. Brighten: Okay. I was like, hold up. Because he is an influencer. Is that what we call?
Dr. Victoria Vargas: No,
Dr. Brighten: he's an
Dr. Victoria Vargas: influencer. I'm
Dr. Brighten: just, he think he's work,
Dr. Victoria Vargas: he fights to remove disease, like, and he fights to remove disease completely.
For example, instead of doing IVF as an option, like you do an, an amazing job on surgery so that patients don't need to have IVF, they can spontaneously conceive [00:40:00] and that's a lot of what he's shown with his work.
Dr. Brighten: Yeah,
Dr. Victoria Vargas: but I mean, I think adenomyosis is under treated or maybe underused with patients and undermanaged.
There's promising things like fu high intensity frequency ultrasound. I at our A A GL this year. Many people were talking about that, and it's not really easy to do here in the us but there's other things coming outta the woodwork for adenomyosis. So maybe in the future you wouldn't even need to be on the pill.
Dr. Brighten: You have to say more about adenomyosis. 'cause you're right, these women, they don't, yeah, they don't get the treatment.
Dr. Victoria Vargas: It's really common with endometriosis. It's, in my experience, I feel like I almost, it's almost a surprise not to see features of adenomyosis on ultrasound for my patients with endometriosis.
So, do
Dr. Brighten: you wanna know what my, uh, reproductive endocrinologist who I fired said to me when I brought in the objective MRI study that showed I had an myosis. He said that's just the new trendy diagnosis like a DHD. And I was like, we're so broken up and you don't [00:41:00] even know it yet. And my husband was in the room during that conversation because I challenged and I said, this is objective finding.
Like, or this is not my opinion, this is not me just coming in like saying I think I have this, like I'm showing you radiologist read this, I have this. And my husband was like, you know, I hear you talk all the time about the gaslighting that happens. He's like, I never really experienced it. And to see, even in the face of imaging that said otherwise, how he just decided that.
No, you are just making this up. And he told me it had no effect on being able to get pregnant. And I was like, I don't know how you got a medical degree. I'm going to leave. Like, and, and that was it. I was gone. That's
Dr. Victoria Vargas: just so incredible. Yeah. It's, it's horrifying. I don't wanna get too tangential on adenomyosis unless you would like to.
Dr. Brighten: We do need to talk about adenomyosis. I mean, it is part of like, I, I was going to bring up, because surgery is very wah w right? Yeah. Because when it's diffuse, what are you Yeah, I mean I have diffuse adenomyosis and it's something that like, people are always like, why don't you get it operated on? And I'm like, okay.
So I'm from California and there's something, a cut of meat [00:42:00] called a tri tip. I'm always, I'm like, you ever see a really good cut of meat and it's got all this fat marbled in it? Yeah. That's what my uterus looks like. So what would happen if you went in and took out all the little pieces of marbled sections?
You just have this floppy no form. Like it's not an organ that functions anymore.
Dr. Victoria Vargas: You know, I think it's just there, just like there are objective criteria to diagnose. Endometriosis using ultrasound. There are objective criteria to diagnose adenomyosis on ultrasound and MRI that are just underutilized.
So it's underdiagnosed. I think in Europe, probably in Latin America, they do a better job because they use these tools that are available to them. It's, it's not that hard to do. Uh, Katerina, kusos, another person you can think about having on your podcast. A lot of people are really experts in imaging, um, adenomyosis, and I think recogni just giving the patient that information that they have, it is so empowering to the patient.
It it, it gives them expectations about. You know, the outcomes of their surgery, the outcomes of their pelvic four [00:43:00] pt, you know, what other adjunctive treatments that might, they might need as a result of having adenomyosis. I just think it's the underdiagnosis is, is very harmful.
Dr. Cindy Mosbreer: I do think that putting a marina IUD in someone with adenomyosis, say if we operate on them when they're 20 or 25, they're not ready to have kids yet, but they have adenomyosis.
I think, and, and I'm not aware of any studies looking at this, but I do really believe that it helps that putting that marina in and having that progestin kind of slow down, the progression of the adenomyosis helps to keep their uterus kind of in the same physiological shape that it's in when they're 20, you know, 5, 6, 7 years down the road when they, when they actually want to get pregnant, as long as they can tolerate it.
Dr. Victoria Vargas: And
Dr. Cindy Mosbreer: some, I think it's maybe 50 50 of the gals with end adenomyosis who will tolerate a marina [00:44:00] and who will not.
Dr. Victoria Vargas: Yeah. But the, there's some studies that in the fertility literature that show like you'll have a higher implantation rate if you do even because they love, they use, this is one area where I feel like Lupron has some data to support its use, but like progestins also have this.
Data to support it, and it, it's a less, it's a more long-term option that's, you know, more viable for these patients. I know it's controversial to use hormonal therapy. I think, I think it's reasonable for adenomyosis, you know, until haifu becomes more widely available or other alternatives are available for it.
Dr. Brighten: And what exactly is haifu and how is it administered?
Dr. Victoria Vargas: So I've never done it, but it's high intensity frequency ultrasound energy, which is like cheap and easy, which is probably why we can't easily do it. I don't know. No one's making money off of it, but, um, you just treat the uterus with this during surgery and it's like, I don't think it's very difficult to do.
Dr. Brighten: Is it a one and done treatment, like you just,
Dr. Victoria Vargas: I believe it is, and probably you could retreat if it, you know, if the treat was in the first treatment was insufficient, there's probably a [00:45:00] way to do it. Again.
Dr. Shanti Mulling: I don't know that it's widely available, but it has also been used to treat. Abdominal wall endometriosis.
Dr. Victoria Vargas: Yeah. And also I think cancer, some cancers ated with it.
Dr. Brighten: Fibro, yeah. Yeah. Fibroids. Yeah. Interesting. Yeah. Mm-hmm. Yeah. And speaking of fibroids, how often are we seeing fibroids as a co-occurring condition with endometriosis?
Dr. Ana Sierra: 85% is really common. It's even where if you are programming a myectomy, a myectomy to not have omes that found them.
Dr. Brighten: So I wanna ask, what are non-surgical interventions that you offer patients that can actually get them relief and buy them some time, maybe before they have surgery?
Dr. Cindy Mosbreer: We just got a machine in our office called the Soft Wave, and it's a, it's a shock wave machine and you can use it on the pelvic floor, you can use it on the vaginal apex, kind of through the bladder.
You can use it on the abdominal wall mostly the PTs use it for trigger points, um, and things like that. And it, it can help PT [00:46:00] be more effective. It can help to release kind of spastic muscles. Um, and it, and it actually works almost like PRP does. So it, it creates an acute inflammatory process that then helps to get rid of the chronic inflammatory process.
Dr. Brighten: And what's PRP for? People who aren't
Dr. Cindy Mosbreer: slightly rich plasma.
Dr. Brighten: And do you ever use that as part of your endometriosis protocol?
Dr. Cindy Mosbreer: Well, I mean, not really as part of the Endo protocol, but we do have the ability to do PRP. So we draw blood, we spin it down, and then we take the layer where the platelets are and the platelets have all these little healing factors.
They have these little inflammatory guys that can do what the. Soft wave does, which is to create an acute inflammatory process that then helps to break down necrotic tissue and then helps the body heal itself. It's kinda like the little brother of stem cell therapy.
Dr. Brighten: I had [00:47:00] it when I had my excision surgery.
I asked him to inject my ovaries with prc.
Dr. Cindy Mosbreer: Yeah. So
Dr. Brighten: I'm like, as long as you're in there and I'm under and I'm sleeping, let's like hook a girl
Dr. Cindy Mosbreer: in. Yeah. So the infertility, there's, there's quite a bit of literature on kind of rejuvenating ovaries and, and raising a MH levels and, um, things like this with PRP for the ovaries.
Mm-hmm. Um, so Nvo sprays it on the bed of the excision area. We use, um, fibrin glute to do that. To pre, uh, prevent adhesions and things like that. But we use PRP primarily, uh, in patients who have, uh, either after hysterectomies, if their vaginal cuff doesn't heal quite right, or if they have vaginal endo that we've removed and there's granulation tissue or things like that at the cuff, we'll use PRP and it usually will take care of that.
Dr. Brighten: Anna, are there any non-surgical interventions for pain management you offer patients?
Dr. Ana Sierra: Uh, [00:48:00] acupuncture does help and has a place. I have the fortune of working with a friend that I met. It's been 100 generations of acupuncturists.
Dr. Brighten: Oh, wow. Yeah.
Dr. Ana Sierra: But he's a, a, a doctor, a medical doctor, and their family is from Taiwan.
But, uh, he was born in Argentina and now he lives in Mexico. He's really good at understanding the pain, uh, because he, that's the reason that he went into medical school to understand what he was doing, and now I think we have had very good results with acupuncture.
Dr. Brighten: Mm-hmm. Vicki, is there anything that you
Dr. Victoria Vargas: offer?
Yeah, I mean, I think along that same vein, I don't think this is the only thing, but I feel like anything that stimulates her vagus nerve. I think helps. Okay, so
Dr. Brighten: you mentioned Vagus Urban episode one and I was gonna make you come back to it too.
Dr. Victoria Vargas: Yeah.
Dr. Brighten: Tell people what vagus nerve is. How do you stimulate it?
Why does it matter?
Dr. Victoria Vargas: It's the biggest nerve in the body, and I should probably say what the vagus nerve is. She's a nerve expert.
Dr. Ana Sierra: Well, I think this, I think is a little bigger, but,
Dr. Victoria Vargas: okay. I say it. [00:49:00] Say what?
Dr. Ana Sierra: No, no.
Dr. Victoria Vargas: Yeah,
Dr. Ana Sierra: go.
Dr. Victoria Vargas: So it modulates the parasympathetic nervous system, which is the relaxation nervous system, and it that modulates inflammation.
So like if, if you have a fight or flight activation or your, you know, your sympathetic nervous system is overstimulated, you have more inflammation. Studies have shown there's like a randomized control trial. From the NIH that showed that patients with rheumatoid arthritis who had vagus nerve simulators implanted, had fewer rheumatoid arthritis flares.
And I feel like one thing that the eastern cultures have that like have known for millennia probably, um, and their like medicinal approaches is that the key to health is to stimulate your vagus nerve. So they do that through acupuncture, yoga, meditation, and so many of the practices that we see from Eastern, uh, medicine is based in.
Stimulating your vagus nerve. Now come to Western lifestyle, especially in the US and it's hustle culture that we have stimulate your [00:50:00] sympathetic nervous system, do CrossFit, release cortisol nonstop. And unfortunately, you know, pain, the pain experience is just so much more heightened and inflammation is so much more heightened from that.
Not to put it back on the patient, but like anything you can do to stimulate your vagus nerve, that means go for a walk in nature, get enough sleep, eat a healthy diet. You know, like be with the people you love, deep breathing meditation, like anything. And I think that is one thing that may help. A little bit,
Dr. Ana Sierra: a teacher explained this to me, like if it was, I would try to flush a toilet when the water is already down, like you flush the toilet and you try to flush it again, there's no water there.
So if you don't wait for the advocated potentials to go back again to the primary, to the main brain of the cell, you're not going to be able to flush again. So you need that relief in order for them to work properly. So some of our patients have like this amount of discharge and discharge and discharge of their sympathetic nerve, and we have to help them regulate.[00:51:00]
Dr. Shanti Mulling: Mm-hmm.
Dr. Brighten: Shanti, any pain management?
Dr. Shanti Mulling: Yeah, so, uh, trigger point injections. So sometimes we talked about central nervous, uh, desensitization. We've talked about vagus nerve calming down, but sometimes this chronic pain results in deconditioning and, and really like overhold of the walls of the abdominal wall and also the pelvic floor.
And so, um, sometimes I'll just do abdominal wall trigger point injections and also vaginal wall trigger point injections when it's indicated. Once, once you start with this deep pain when you're. A teenager and you go through Menarchy, your whole body becomes somewhat more tense. And so if they're waiting for surgery, not sure you can get some relief through trigger point injections.
And similar to getting body work,
Dr. Brighten: what are you injecting?
Dr. Shanti Mulling: I usually inject Marca long-acting lidocaine solution. Studies show that injecting steroids is not necessarily [00:52:00] more effective. And also studies show that dry needling can give you a similar benefit. But I, I think patients feel an immediate sense of relief when you actually inject them with a lidocaine type.
Dr. Ana Sierra: Don't inject steroids. Don't, uh, steroids. No. The cause a lipotrophy into the myelin membrane so the pain comes back harder.
Dr. Shanti Mulling: Perseverate pain. Yeah.
Dr. Ana Sierra: If you have patient that has, uh, the pain increases whenever they're standing straight and the pain releases when they are flexing because they're flexing their leg and they're releasing their SOAs.
Yeah. Gen FMS nerve goes through the SOAs. Yes. So if you look in the ultrasound for the Gen fms and block the unit femorals, it'll give them a larger amount of relief. That's sometimes just going to trigger points. Yes. I will advise to go through the ilio or ilio hypogastric nerve or the genetic femoral nerve in the.
Ball.
Dr. Shanti Mulling: Yes.
Dr. Ana Sierra: So how bare relief, that's been my impact.
Dr. Shanti Mulling: Yes. Lovely.
Dr. Brighten: [00:53:00] Vicki, I wanna ask you, for patients who are in pain, they're trying to seek help from a provider, what's a way they can categorize and quantify that pain to get their provider to listen?
Dr. Victoria Vargas: I like what Anna was saying about the five Ds. I mean, that's how I collect the information.
I'm like, which bodily? Systems, is this impacting bowel, bladder, sexual function? Um, p pain with periods, pain between periods? Where is it? Um, what's the quality of it? You know, what, which ones are at which part of your cycle? I'm like a, an investigator interrogator. I ask so many questions from my patients.
Um, I think some people's like coping mechanism is ignoring it and they like get a little intimidated about having to think about all these. Details, but I'm, and that's not my intention at all, but like, if, you know, some patients know every detail and they're so grateful to like, tell someone about it and have them listen.
But yeah, I mean, basically I just wanna know all the details about your pain. So,
Dr. Brighten: so where's the pain? What's the quality? Yeah. Is it sharp? Is it burning? [00:54:00] Is it aching? Yeah. Where is it at in your cycle? What about activities of daily living?
Dr. Victoria Vargas: Yeah. I wanna know the systemic symptoms too. Not just the pain activities of daily living.
What is it impacting? Um, and honestly, like, you know, those details help me a lot. The ultrasound helps a lot. I, you know, I, I contact my friends when I don't know, like, I'm like, there's this symptom that's really bothering this patient. I don't fully understand it. I'll call Anna, Anna knows I've contacted her about patients and I, I've called Shanti, Cindy, I contact Cindy all the time.
You know, I think, um, the symptoms that the patient has, the ones that are most impactful for them in their lives, like we need to understand them fully, where they're coming from. You know, the only way to do that is just to collect like, as much information as possible. And when it's beyond my expertise, I go to my friends who know more.
Dr. Brighten: Okay. And so if someone's bringing all this data to their provider and their provider is still being like, it's spirit pain, it's normal, is there a phrase or anything they can say that [00:55:00] might get that provider to like, snap into it, maybe leave the last patient behind and be present in the room here and get this person the help they need?
Dr. Victoria Vargas: Maybe I'm too passive, but I'm like, you know, it's, maybe we
Dr. Brighten: should ask Cindy.
Dr. Victoria Vargas: I'm like, when you get, when you get someone on the phone that clearly doesn't wanna help you, you're, you're like, let me call back later and get that per that right person on the phone. Yeah. That's how I see it. You know, like, let me find someone who wants to hear.
Dr. Cindy Mosbreer: And if you go to a gynecologist and they don't wanna listen to you about your pain, they're not gonna do you Right. If they operate on you. Mm
Dr. Brighten: mm
Dr. Cindy Mosbreer: Yeah. And so you don't wanna see that person. You want somebody who's, who is interested enough in what's going on with you to think long and hard about what are we gonna do if we go to the or, what are we gonna find?
What might we find? I mean, I wanna know in advance everything to expect when I get to the or, which is why I spend 15 minutes on an ultrasound for every single patient I see. And, [00:56:00] and I don't wanna be surprised, but it's, it's the doctors that don't wanna talk to people about their pain, they don't wanna recognize their pain.
And the patients are like, how can I get them to, you know, pay attention to me? Well, even if they did pay attention to you, they wouldn't know what to do once they got in your belly. So you just need a different doctor.
Dr. Brighten: So I'm gonna, I'm gonna, I'm gonna push back on this because there have been states, now there's counties in the US that don't even have gynecologists and there are gatekeepers that are PCPs that these women need to take their pain seriously to make the referral so that when they make that three hour drive that to the specialists, their insurance actually covers it.
And so I think, you know, I hear what you're saying. I wouldn't let that person touch me either, but I think that is something we just have to name. We don't, we don't necessarily have to solve it in this podcast, but we have to name it so that patients know that, like we are aware that is very difficult to get to a provider that is, is worth [00:57:00] seeing for your pain.
I
Dr. Cindy Mosbreer: think the physical therapist and the naturopaths know who to send people to, isn't My office gets more referrals from those two classes of providers than they do from any MDs.
Dr. Brighten: Yeah,
Dr. Cindy Mosbreer: all, all of them put together.
Dr. Brighten: We talked about the thoracic, um, endometriosis and Shanti. I'm wondering if there's a breath or posture change that people can make that can help support them if there's a diaphragm endometriosis involved in their case.
Dr. Shanti Mulling: That's a beautiful question. Uh, I don't know of one. Um, but I, I love that idea. I, I'll think about that.
Dr. Brighten: We're gonna have to chime in on it. If you are a physical therapist, I bet you have the answer. And if you could leave it in the comments, um, you know, in you on YouTube is probably the best place. And then that way patients can go and see your answers and also know who's an amazing physical therapist to go see.
So, Cindy, I wanna ask you, true or false endometriosis can always be [00:58:00] managed by stopping ovulation with the pill, using medications like Lupron or taking progestins.
Dr. Cindy Mosbreer: No, of course not. Um, I think we have to individualize our patient care. For every patient, but especially women with endo. Mm-hmm. And, you know, figure out together what works, what they want, what, you know, what can we try, if this works great, we can keep going down this path, but if this doesn't work, then we go this way and then we, you know, we keep trying.
Dr. Brighten: That's what I was really hoping you would underscore, is that individualized care is the best care from the endometriosis patient, not necessarily just one treatment. So, Ana, how do we explain nervous system regulation to patients in a way that isn't telling them that their pain is just in their head?
Dr. Ana Sierra: First of all, you have to validate and you tell them that, one, you believe in their pain. Two, their pain is real because the experience of the [00:59:00] pain is going to be real for them. Even though the origin is in their head. You have to explain them that precisely that, that if they're, they have a centralized pain, they're, they're gonna feel the same way.
There is a book, it's called, uh, diary of the Pain, and it's about a fibromyalgia patient. She explains pain as if it were a presence of someone that she has to share their body with. And she explains, uh, having something is like a constant presence and that makes her never alone. And when you think about that and the ways that it changes their reality, their marital status, everything, you have to be compassionate about them and explain them.
This is another symptom of your endo, and there's nothing in your head. I mean, there's something in your head, but there's nothing wrong with you. And we can manage the symptoms and we believe in you. You have to validate that.
Dr. Brighten: What do you wish partners of endometriosis patients knew about this [01:00:00] pain?
Dr. Ana Sierra: I often explain them, for example, when the ovaries are attached to the uterus or in the, attached to the pelvic wall, I tell them, okay, how about if I staple your, uh, scrotum to one of your legs?
Do you think you'll feel any pain at all? So that's one of the, so they're like, oh, yeah, can, so she has that. I, I usually make them like a drawing of how they are, the how, where they're the ovaries and how they're placed and where is the nodule in their bowel and stuff. And when, when you're talking to them, they have, like, some of our patients have an excellent partners and do help them and do understand them.
But in, in other states or other patients that I have tried or treated most of them as they are not longer good for reproductive, uh. Features or reproductive, uh, functions, they leave them because that's the point of getting married. So it's, it's hard for [01:01:00] women.
Dr. Brighten: Mm-hmm. Vicki, I wanted to ask you, 'cause our next episode coming up is gonna be about surgery, but for women listening right now, who should be on the endometriosis team other than the surgeon?
Dr. Victoria Vargas: So I think we touched on some of them. Like, you know, pelvic floor physical therapists are our friends. I have several acupuncturists that I work, you know, I send patients to and who actually send patients to me. Um, there's some naturopathic doctors that, you know, we collaborate with. Um, anyone else that you guys would add to that?
Dr. Cindy Mosbreer: Uh, interventional pain management.
Dr. Victoria Vargas: Yes.
Dr. Ana Sierra: Psychologists, psychiatrists, multidisciplinary team means. It's our, and nobody has the full picture that you have to work as a team in order for the patients to feel better.
Dr. Victoria Vargas: And I wanna add, if you're lucky enough to have a, like a good radiologist or someone radiology.
Yes, that would be great.
Dr. Shanti Mulling: And then radiologists can also sometimes clear fallopian tubes, uh, interventional radiology. But of course we've talked about [01:02:00] diagnostic, but also functional medicine provider who can really delve into nutrition and work with very specific supplements, work with specific diet, work with food sensitivities,
Dr. Brighten: the mast cell activation.
Dr. Shanti Mulling: So many of our patients have mass. Cell activation syndrome. So many of our patients have, yes. As well as, um, er
Dr. Brighten: Yeah. I would add on the team is a dietician, a nutritionist, someone who doesn't just understand endometriosis, but understands that perfection is never the goal when it comes to eating. And so I really want everyone who's listening to take away from this, that it does take a multidisciplinary team.
You know, for years I'd have patients come to me and I'd be like, okay, we need to get you to the endo surgeon. And they're like, but why? That's why I'm seeing you. I'm like, because we always want their opinion. And I think the same way as a psychiatrist, as other providers and when we need them most, we don't wanna be in an emergency situation scrambling to find [01:03:00] who's the best person for you.
When we could have done that, when you were filling. Pretty okay, so I appreciate this conversation so much. Next, we are talking in depth about surgery, why choosing the wrong surgeon can be the most devastating mistake of your life. So thank you all so much for being here with us. Thank you all for sharing your expertise, and we will see you all in the next episode.