


Testosterone is having a moment—but much of what women are being told about it is incomplete, oversimplified, or outright misleading. If you’ve been told testosterone is only about libido, or that your fatigue, emotional flatness, loss of motivation, or inability to build muscle is just “getting older,” this episode challenges that narrative. In this conversation, Dr. Jolene Brighten breaks down what testosterone actually does in women’s bodies during perimenopause, why symptoms matter as much as labs, and how poorly matched hormone therapy can lead to side effects that leave women feeling worse instead of better.
This episode is a deep dive into testosterone hormone therapy in perimenopause, designed to help women—and clinicians—understand how to evaluate symptoms, interpret labs with nuance, and choose treatment approaches that respect the entire hormone system. Rather than pushing testosterone as a cure-all, this episode lays out when it helps, when it harms, and why careful dosing, delivery method, and monitoring are essential.
What You’ll Learn About Testosterone Hormone Therapy in Perimenopause
In this episode, you’ll learn why hormone therapy in perimenopause requires far more precision than most women are offered—and how testosterone fits into that equation without being oversold or misused.
You’ll hear insights on:
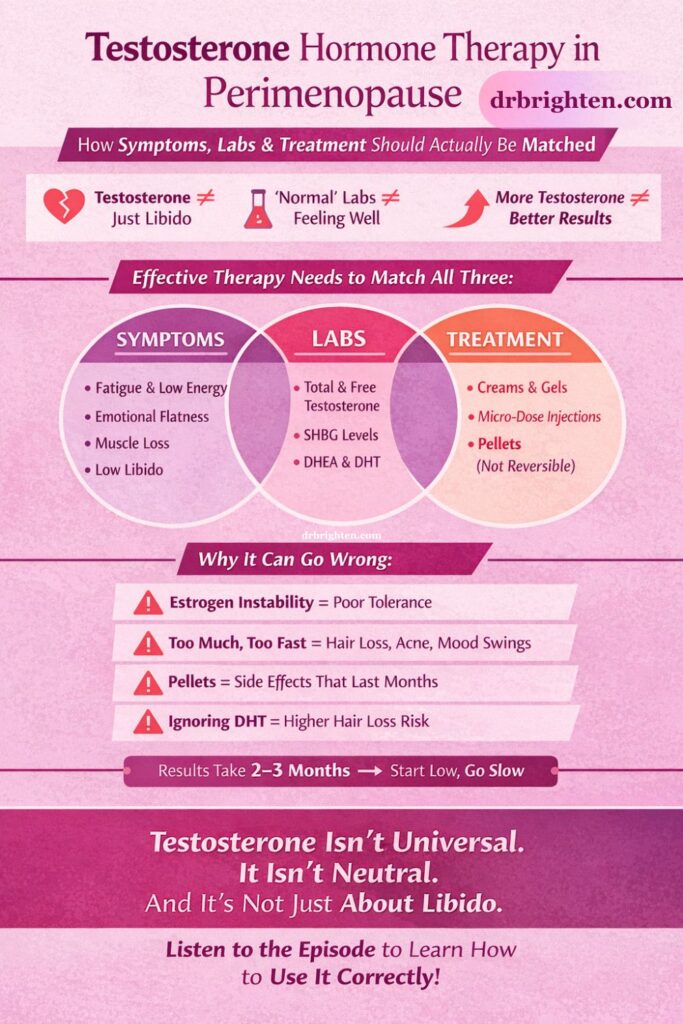
- Why testosterone is more than libido and how it influences mood, motivation, executive function, muscle, and nervous system regulation
- The overlooked reason many women feel emotionally flat, unmotivated, or mentally exhausted despite “normal” labs
- How fatigue despite doing everything right can point to testosterone issues—not burnout or laziness
- Why women in perimenopause often lose muscle mass despite consistent strength training
- The connection between low testosterone and executive dysfunction, including difficulty starting and finishing tasks
- How genital blood flow and sensory responsiveness depend on testosterone—not estrogen alone
- Why some women feel calm and focused on testosterone therapy while others feel angry, impulsive, or wired
- The real risk of supra-physiologic testosterone dosing, including hair loss, acne, voice changes, and facial masculinization
- Why pellet therapy is not reversible and what that means if side effects occur
- How estrogen instability in perimenopause can make testosterone therapy feel ineffective or poorly tolerated
- Why labs alone do not diagnose testosterone deficiency in women
- The critical role of sex hormone-binding globulin (SHBG) in hiding testosterone from tissues
- How DHT and 5-alpha reductase activity influence hair loss risk before starting therapy
- Why women often experience testosterone decline before estrogen even drops
- How ADHD and neurodivergence change the way testosterone therapy should be approached
- The FDA’s narrow approval of testosterone for women and why most clinical use is technically off-label
- Why starting low and going slow is non-negotiable in hormone therapy for perimenopause
- How long testosterone therapy actually takes to work and why impatience leads to side effects
Hormone Therapy in Perimenopause: Understanding Testosterone Beyond Libido
Hormone therapy in perimenopause is often framed as an estrogen conversation, but that leaves out two hormones that frequently decline first: progesterone and testosterone. Testosterone production in women begins to decline as early as the late twenties, and for many women, symptoms appear long before menopause is ever diagnosed.
Testosterone plays a foundational role in women’s health, influencing:
- Mental drive and motivation
- Emotional resilience and mood stability
- Physical strength and muscle maintenance
- Sexual desire, arousal, and orgasm
- Nervous system threat perception and stress tolerance
When testosterone is low, women may become hypervigilant, anxious, or easily overwhelmed—not because they are “too sensitive,” but because the body is compensating for a perceived loss of physical and neurological resilience.
One of the most important takeaways from this episode is that testosterone therapy must never be evaluated in isolation. Estrogen fluctuations during perimenopause can make testosterone therapy feel ineffective or destabilizing if estrogen is not addressed first. Likewise, inflammation, HPA axis dysregulation, and insulin resistance can all suppress testosterone production—meaning supplementation may not be the correct first step.
Lab Testing for Testosterone in Perimenopause
There is no universally accepted laboratory definition of testosterone deficiency in women. Blood levels do not reliably correlate with symptoms, and many women feel unwell despite being told their labs are “normal.”
In this episode, Dr. Brighten explains why a complete testosterone panel matters, including:
- Total testosterone
- Free testosterone
- Sex hormone-binding globulin (SHBG)
- DHEA-S (adrenal contribution)
- Dihydrotestosterone (DHT)
Each of these markers tells a different story. For example, elevated SHBG can bind testosterone so tightly that free testosterone remains low—even when total testosterone appears adequate. High DHT may signal increased risk of hair loss or acne if testosterone therapy is initiated without addressing conversion pathways first.
Testosterone Delivery Methods: What Women Need to Know
Not all testosterone therapies are equal—and the method of delivery matters profoundly.
This episode breaks down:
- Topical creams and gels, which allow for easy titration but require daily adherence and careful handling to prevent transfer to children or pets
- Micro-dosed injections, which offer predictable absorption but can cause mood swings due to peaks and troughs
- Pellet therapy, which is long-acting but not reversible and carries a higher risk of prolonged side effects
- Oral testosterone and troches, which are generally avoided due to metabolic and liver concerns
A recurring theme is that reversibility matters. Side effects from testosterone often take months to appear—and months to resolve. This is why escalating doses too quickly or choosing irreversible delivery methods can lead to regret.
Who Benefits Most From Testosterone Therapy in Perimenopause?
Women who are most likely to benefit from testosterone hormone therapy in perimenopause often share a combination of:
- Persistent low mood not tied to cyclical hormone shifts
- Fatigue despite adequate sleep, nutrition, and exercise
- Loss of muscle mass or inability to build strength
- Reduced motivation, drive, and follow-through
- Low sexual desire or muted physical sensation
However, testosterone is not neutral and not universal. Women with certain sensitivities, inflammatory conditions, or estrogen instability may require additional support—or may need to address root causes before initiating testosterone therapy.
This Episode Is Brought to You By
Dr. Brighten Essentials Radiant Mind — a science-backed formula created to support women’s brain health through every stage of life. If you’ve ever felt the brain fog of perimenopause or noticed how ADHD can amplify challenges with focus, memory, mood, or sleep, you’re not alone. Radiant Mind combines clinically studied saffron extract, Bacognize® Bacopa, Cognizin® Citicoline, and zinc to help nourish your brain chemistry and support clarity, calm, and resilience.
Sunlighten Saunas — Want a gentle, science-forward way to sweat, recover, and unwind? At Sunlighten, infrared saunas deliver soothing heat that supports relaxation, muscle recovery, and deep, comfortable sweating—without the stifling temps of traditional saunas. With low-EMF tech and options for near, mid, and far infrared, you get a calm, restorative session tailored to your goals.
Exclusive for podcast listeners: use the code DRBRIGHTEN to save up to $1,400 on your sauna
LUMEBOX
Ready to take your skincare results to the next level—right from home? 💡 LUME Box delivers professional-grade LED light therapy in a sleek, easy-to-use device that targets fine lines, pigmentation, and dullness at the cellular level. Just minutes a day can help boost collagen, calm inflammation, and reveal that lit-from-within glow. It’s the same science trusted in top dermatology clinics, now in your hands.
Shop now use code drbrighten for our exclusive community discount on your purchase.
Links Mentioned in This Episode
- Perimenopause hormone support plan
- Episode on evidence based ways to boost testosterone naturally in women
- Hair loss protocol episode
Considering testosterone therapy in perimenopause? Listen before you start so you understand dosing, delivery options, and the side effects no one warns you about.
Frequently Asked Questions About Testosterone Hormone Therapy in Perimenopause
Testosterone therapy can be safe when appropriately dosed, monitored, and matched to symptoms and labs. Risks increase with excessive dosing, poor monitoring, or irreversible delivery methods.
Poor tolerance often occurs when estrogen is unstable, dosing is too high, or testosterone is introduced without addressing inflammation, cortisol, or insulin resistance.
Yes. Elevated DHT or increased 5-alpha reductase activity can contribute to hair loss, particularly if dosing is excessive or conversion pathways are not assessed beforehand.
Most women do not experience full benefits until two to three months of consistent use. Side effects may also take months to appear.
Pellets are not inherently unsafe, but they are not reversible. If side effects occur, they may persist for months, which is why many clinicians prefer reversible options first.
Yes. Testosterone plays a role in executive function, motivation, and mental stamina—but only when appropriately matched to the individual’s hormone landscape.
No. Symptoms often matter more than isolated lab values, especially given variability in receptor sensitivity and binding proteins.
Transcript
[00:00:00]
Dr. Brighten: We gotta have some real talk because if you've been told, your testosterone is only about your libido, you have been given an incompliant and frankly, misleading story. And the perpetrators of that, um, tend to be the medical community and FDA I'm looking at you. So the symptoms that suggest that women may benefit from testosterone are often misattributed.
They're dismissed and they're labeled as things like. Burnout, , depression, just getting older. Um, have you tried losing weight? I think these ridiculous things that we are told is women, instead of somebody just digging deep and figure out what's going on with our hormones. So today we're talking about the patterns that actually raise my clinical eyebrows when a patient presents with these symptoms. But
I want you to stick around because I am gonna go through the types of hormone therapy that are available to women. What you should know, pros and cons. And we're gonna go through lab testing.
If you recognize yourself in any of these symptoms, I'm about to list, then this episode is for you [00:01:00] if you feel emotionally flat or have a persistent low mood. I'm not talking about cyclical, we're not talking about A-P-M-D-D picture, we're talking about most days outta the month. You just feel kind of bluesy, a bit sad, less motivated. If you're also having fatigue despite doing everything right, you're taking your B vitamins, you're exercising, you're getting eight to nine hours of sleep if you are a good job.
But everything right is still not giving you the energy that you need. When it comes to your muscle mass check in right now are your muscle gains matching the effort you're putting in? If you're losing muscle or you're unable to build muscle, despite consistent strength training, not just like every now and again, we go to the gym, okay, consistent, then we start thinking about testosterone. And that's not to put you down if you're not being consistent. It's just to say if you're not consistent and you're not building muscle mass, that would make [00:02:00] sense. If you feel you have a loss of drive, motivation, follow through, you don't wanna start a project, and if you do muster the energy to start a project, you cannot follow through on the project.
So that difficulty initiating or completing tasks, this is because testosterone affects our executive function. Again, testosterone is far more than our libido and our ability to please men, which is kind of the view and the take that the FDA has. Now if you're having low sexual desire, so you're not interested, you're less responsive to, uh, stimuli. So whether that be, uh, mental or physical stimuli that can be related to your testosterone as can reduce genital sensation, inability to achieve an orgasm can be related to our hormones as well. now libido and women's sexual health is far more than just hormones.
It's far more complicated than that, but these hormones do play a [00:03:00] role, for example, difficulty getting aroused and the achieving of an orgasm that can be hormonally related. So anytime somebody says, Hey, I've got these sexual concerns, I'm gonna look at their hormones, but I'm gonna look at a full picture as well. Now, if you find that you don't have the drive, the ambition, the ability to set boundaries like you used to, that can be another sign that testosterone is getting low. If you feel like your nervous system is on edge all the time, you're always panicking. Every little thing is perceived as a threat that is your body's way of keeping you safe.
Because of testosterone's low and we are weaker, then we better be hypervigilant about our environment. So if any of these sound like you, I definitely want you to stick around because I think it's so important that women understand testosterone in their own body. Testosterone plays a crucial role in our genital blood flow. It's not just estrogen involved There. Sensory, responsiveness, motivation, and drive, not just sexual, like drive [00:04:00] all together that ambition, that like wake up, kick ass, repeat kind of drive. And before we get into labs and testosterone hormone therapy in women, quickly, if this show has helped you think differently about your hormones, please consider subscribing, dropping a comment, leaving a review, sharing this with someone who needs this information. This can seem like such a small act, but it is tremendous in supporting this show.
And if you're new here, welcome to the Dr. Brighten Show. I'm Dr. Jolene Brighten. I'm board certified in naturopathic endocrinology. I have been supporting women and prescribing hormone therapy for about 15 years now. And in addition to that, I'm a nutrition scientist. I'm a sex counselor, and I'm certified menopause practitioner.
So when we talk testosterone therapy, that is totally my wheelhouse and I brought notes today.
If you are a woman and you're paying attention, you know testosterone is having a moment right [00:05:00] now and women are finally in masses hearing that it's not just a male hormone that ovaries make it. And that it affects your energy, your muscles, your libido, and your brain function and all of that is progress.
And as someone who has been in this arena long enough to have been criticized because the Women's Health Initiative was out there telling everyone that hormones would hurt us and I was prescribing them at the time, I, for 1:00 AM so happy to see this. Now, the problem that's happening at the same time that I need to put you onto is that testosterone is being oversimplified.
There are providers who are like, cool hormones are great. Women need hormones. Let's put everybody on hormones. And in some instances, testosterone's being oversold over-prescribed, and it's being done. Poorly, and that comes with risks, and that does cause harm. And so as exciting as it is, I wanna give you some guidance today so that you don't fall into the trap of [00:06:00] being given super physiological levels of testosterone.
Some providers do that, but hair lines start to disappear. They start receding, voices start to drop. There's a masculinization of the face, like the, your body becomes very, very muscular. I love that. I love seeing muscles on women, but it's the type of muscles that you don't get without having hormonal influence to push you there.
And listen, if you are someone who has low testosterone, I want you to know I'm not a gatekeeper, okay? I'm not talking about this from a, a perspective of like, we should not be giving women testosterone. Hell, yes, we should give every woman who needs testosterone the option to choose for herself if she wants to use testosterone.
We're gonna talk about who benefits from testosterone, who needs to be cautious, and how testosterone fits into the larger hormone system But first I wanna get into labs and before we go through labs that should be tested before prescribing testosterone, I wanna remind you, I have a plan for you [00:07:00] that guides you through how to eat, how to move, how to sleep, how to reduce stress, how to do everything your body needs to optimize your hormones through midlife.
If you go to dr Brighten.com/plan, D-R-B-R-I-G-H tn.com/plan, you can grab that meal plan. Recipes that don't require too much cooking helps you hit your protein and your fiber requirements to have optimal hormones every day and gives you guidance on how to work out. Okay, labs. First thing we gotta do is be very clear that labs alone, do not diagnose a testosterone deficiency in women. You cannot look at labs alone and not also ask the patient questions and understand how it fill to live in their body.
And keep in mind, you know, we've gotta do a whole panel with testosterone, but total testosterone does not equal tissue level testosterone normal doesn't mean that you feel great in your body. Okay? I really hate when people have symptoms and then they're like, but my doctor said all [00:08:00] my labs are normal.
And I'm like, is it normal based on the, the reference range that's based on elderly people and sick people? 'cause that's the majority who get labs drawn. Like that may not be normal. It's also important to understand, as we talked about in the last episode, that receptor sensitivity matters. So when it comes to lab testing, there's a lot of nuance and often I will see that doctors are just ordering a total testosterone, hanging their hat on that and saying, okay, that's it.
End all, be all. Your total testosterone looks fine. But I do things differently and I get a full panel. And I definitely would recommend that you do the same. And if you are someone who has been told your labs are normal, therefore your symptoms don't matter. Wrong. When it comes to hormones, symptoms matter more than just a single number. We have to look at an entire picture.
so when it comes to testosterone testing, the panel that I order for patients is a total testosterone. That's gonna tell me how much you're making a free testosterone. That's gonna tell me how [00:09:00] much is bioavailable a sex hormone binding globulin? That's gonna tell me, are you binding up that that testosterone, and is that the reason why your free testosterone is low, is that we've got a protein problem there?
I also look at DHA sulfate that tells me how much the adrenal glands are contributing and doing their role. Right? Remember from our last episode, we women primarily make testosterone from our ovaries and our adrenal glands. And then I also like to look at dihydrotestosterone or DHT. Now you can do all of this in a serum lab.
You can also do a Dutch test and then do blood work for the sax hormone binding globulin. The DHT tells me how active is your five alpha reductase activity. That's an enzyme that takes your testosterone. To a very potent form that leads to hair loss, sometimes oily skin acne. And then next to hair loss being the worst is hirsutism, and that is growing hair where you do not want it.
So I wanna know that [00:10:00] ahead of time, because if I'm gonna prescribe testosterone, I wanna get ahead of things in that pathway and make sure that I don't push someone into losing their hair because then they would hate me forever, and I don't want that. By the way, if you are losing your hair, I have a whole hair loss protocol episode that I will link to in the show notes.
There'll [email protected], or they will be below this episode in YouTube so that you can get some solutions and grow your hair back. Now something else that's like really, really important to understand is that there's no defined testosterone deficiency syndrome in women. That's just based on labs that we can just look at the labs and say, oh yeah, absolutely. Like this is what's true for you. In fact, studies have looked at testosterone levels in women, in perimenopausal, women in, uh, postmenopausal women, women using testosterone therapy, and it has really, there's really been no consensus.
And in fact, what we see is that the blood markers don't always correlate to how you're feeling and how you're [00:11:00] feeling may not be showing up in the lab work. So it can be a bit tricky. That's why I look at the full panel because a lot of times these studies, they'll just look at total testosterone or maybe just free testosterone and like they're not looking at the full picture, like, how is the adrenal function?
Testoserone Therapy - Front:
So the choice to use testosterone therapy for clinicians is based on clinical judgment and married with the labs. So we're gonna look at the labs, we're gonna look at the patient's symptoms. We're gonna understand what is happening for this entire person. Remember in the last episode, I'll link to that too 'cause I'm acting like you heard it, but maybe you didn't hear it.
I talked about how inflammation, um, that can be impacting testosterone levels. So we don't wanna go chasing testosterone when the root at all of that is cortisol. HPA dysregulation happening and we're having inflammation, like we need to address the inflammation. And maybe testosterone is a part of that, but it may not be, and it may be the wrong mood to try to push [00:12:00] testosterone when what we really need to do is drop the inflammation.
Now, in terms of lab values, there are certain parameters I am looking for, but I just don't want
Testosterone Therapy - Side: Uh,
Dr. Brighten: any clinician who's listening to only see a patient as their labs. And I also don't want you as the individual to be like, oh, okay, these labs mean I have to get on testosterone.
It is much more nuanced than that. Now when it comes to total testosterone, I like to see a level of at least 15 nanograms per deciliter. These are the lower ends of the range, by the way that I'm looking for. If you have symptoms, it's gonna change things on how I look at it. But if it's less than 15, I'm like, we gotta production problem.
If we have a low sex hormone binding globulin. I'm looking for insulin resistance. I'm looking for inflammation. So this is very common in the polycystic ovarian syndrome picture. If I see a high sex hormone binding globulin, then I expect to see [00:13:00] a low free testosterone, and that is common on oral estrogen.
So hormonal birth control, we talked about in last episode, thyroid excess. Um, if you have what is called estrogen dominance, so we have too much estrogen going on, can even be xenoestrogen. Sex hormone binding loin goes up. It's a protective mechanism by the body to keep you from getting overexposed to estrogen.
Also testosterone. So it's protective, but it can really suck when you are like dealing with low testosterone symptoms now for free testosterone. If that's below one I'm, and I'm looking at sex hormone binding globulin, and that looks normal, but total testosterone is below 15. I'm like, we are not producing testosterone.
We are not converting testosterone. Ideally, a free testosterone should be between two and four, so below one with symptoms, eyebrows go up. We need to be thinking about what we want our next step to be. Maybe it'll [00:14:00] be working on those adrenal glands, but it's likely gonna be GHEA or testosterone therapy if somebody is in perimenopause. Now we mentioned DHEA sulfate. That is a very age dependent number and it depends on how you're measuring it. Are you doing blood spot? Are you doing blood draw? Are you doing Dutch panel? But DHEA sulfate, that's specifically what we're looking for. It helps distinguish adrenal versus ovarian contribution.
And so if total testosterone free testosterone low, D-H-E-A-S is low sex hormone binding globulin is normal. We've got an overall production issue and testosterone, as I talked about in the last episode, it can decline starting in your late twenties. Uh, testosterone is on its way out and sometimes it's going out before estrogen even is.
And so that's what's kind of lame about perimenopause. Everybody talks about estrogen, but they forget the fact that progesterone and testosterone can go first. Now, DHTI [00:15:00] always, I just want to plug that again. Hair loss and acne. We want to avoid those side effects, so that should be part of a FA panel as well.
If your DHT is elevated, like, Ooh, five alpha reductase is off the chain, that enzyme is just cranking, cranking, cranking. Taking your testosterone to is not all bad. Okay? We need it, but too much of it. And then we're like, where is my hair? Where did my hair go? And I never want that for you. Now, as I mentioned before, we need to have a balance of hormones because when estrogen is unstable, it's rising and crashing in perimenopause. Testosterone therapy can be poorly tolerated if we don't get your estrogen right before testosterone therapy.
Um, testosterone therapy doesn't feel like it works, but also we might see metabolic changes. We don't like. We might see more belly fat, so we have to get, we have to look at your estrogen as well. We gotta look at your symptoms and maybe we're gonna do blood work, and I will link to other episodes on that.
But the takeaway is testosterone is [00:16:00] gonna work best when estrogen is more stable. And this is why we don't give testosterone in isolation. We don't just look at testosterone only. Okay, we're gonna talk about who testosterone is most likely to help. But before we get there, please stick around to the end because I am gonna go through the different forms of testosterone and what you should know before starting testosterone therapy.
Testosterone Therapy - Side: So
Dr. Brighten: the FDA is like, listen, if you've got low libido, you are not in the mood. Uh, you know that like your desire is distressing you. Okay? So it's not just that like, oh, I'm not really in the mood. It's that like I'm in the mood and it's stressing me out. Okay? You can have testosterone right now. There is no FDA approval for all of the other ways that women suffer when they don't have enough testosterone.
I said we weren't gonna do outrage, but it's kind of, I'm like a little bit pissed off about it. So here's the thing. Your testosterone labs look low and you're feeling depleted. You are in your forties, okay? So you are likely in [00:17:00] perimenopause, you are having executive dysfunction. So that is like your mental drive, your stamina, your starting projects, your following through.
None of that's working for you anymore. Um, if you have a DHD and that's happening for you, like definitely testosterone's, like a forgotten one, uh, for A DHD women, and I can do a whole nother episode about the nuance about that because testosterone therapy is way more nuanced in an A DHD and autistic individual than it is in a neurotypical woman.
So far we have covered the lab testing and who would be a good fit for this? We went over all the symptoms at the top of this. If you're having those, you're labs are showing that you're low, you're probably a good candidate for considering testosterone therapy. Now I want to move into the types of therapy, so please stick around for that.
But before we get there, I need you to understand this. The FDA has only approved testosterone therapy. [00:18:00] If you have low sexual desire and it's stressing you out, then the FDA is like green light go. A lot of critics will say, if you are using testosterone therapy for anything other than this distressing low libido symptom picture, you are using it off label.
And we're not supposed to do that. Well, I hate to break it to you, but spironolactone is not meant to treat PCOS, cystic acne, oily skin hair loss, uh, you hirsutism, but we do it right. There are a lot of drugs that we use off label and so to gatekeep and say, well, you can't use testosterone because it hasn't been FDA approved.
I hate to break it to you, but the majority of ways that we are using drugs these days, they are off-label uses. So they don't always go back and say, okay, we're gonna re, we're gonna seek FDA approval for this. They will have off-label uses. So as of right now, there's no testosterone product that's actually approved for [00:19:00] women, despite the FDA saying, Hey, if you're not in the mood and it's freaking you out, you can have it still.
We don't, we don't actually have, uh, any testosterone. So every form of prescribed testosterone is off label because. It was designed and dosed for men, and then we've had to adapt it very carefully for women. Now, caveat, I can use a compounding pharmacy and then get the dose exactly the way I want it for a woman, but that's pricey.
And not everywhere has a compounding pharmacy. So there are limitations to that. And before anyone comes in and says, oh. Compounding pharmacy drugs are not FDA approved. Let me just stop you because that's a lie. That is actually willful disinformation to dissuade you from using a compounding pharmacy, usually by clinicians who are not actually trained in hormone therapy.
So I was actually trained in medical school in hormone therapy, unlike other doctors, and they don't know how to compound medications. So because they don't know [00:20:00] how to compound medications, they tell you it's dangerous because that protects what they're doing in their practice and helps keep them elevated on a pedestal as the expert and helps draw a line in the sand of us versus them.
Compounding pharmacies use hormones that are approved by the FDA, the FDA approves medications that are meant for going out into the general population. When I compound something just for you, I make it just for you. There is no reason to have the FDA approve that, that's not the role of the FDA. The FDA doesn't care about the titrated fine.
Um, you know, prescription that's fine tuned to the individual. They don't care about that. That's not what they do. That's not even in their scope. Their scope is, is the testosterone. You're using FDA approved. Yes. That is what's safe. So it is FDA approved, but the way we compound it isn't meant to go [00:21:00] out to the whole population that qualifies for that.
So it doesn't need to be FDA approved. And I think that nuance is really important because I, you know, the rhetoric I've seen around this. It is willful disinformation. I mean, perhaps maybe they just don't understand how the FDA works. They certainly, a lot of these people don't understand how hormones work.
They did. They received training in the birth control pill, placing an IUD in pregnancy and then called themselves hormone experts, but never received training in actually working to fine tune women's hormones naturally. That's why when you have period problems, all they give you is the pill. You have hormone related problems.
You get the pill. You go into perimenopause and they're like, yeah, just take the pill. I, I just can't with that. Women deserve so much better.
Okay, rant over. Let's talk about what you need to know before going into testosterone therapy. So first thing is women need tiny, tiny physiological [00:22:00] amounts, okay? Small dosing errors matter absorption. Variability matters. Reversibility matters, timing matters. And you need to understand that benefits often take two to three months.
I don't ever wanna catch any of you, and certainly not my patients. I always warn them of this, It is just because we get you going on like five milligrams a day and after a couple weeks you don't fill it. And then you're like, well just do it twice a day.
And then I catch you like two months later and you're like, why am I breaking out and what is happening? And I'm like, yeah, what is happening? Don't ever decide to dose up yourself. Okay? Please don't ever do that because side effects take time to emerge. And it may be a couple months before you notice side effects.
And then it's gonna take a couple months for those side effects to resolve and go away. That's why we always start low and we go slow. I'd rather you feel a little bit better and get impatient with me than us. Like punch through the ceiling of your tolerance and then you hate me because you're like, why do I [00:23:00] look like a teenage boy?
But I'm starting to bald like a middle aged man. Like what is happening here? So we don't ever escalate in a few weeks just because someone doesn't feel it yet. It is not uncommon to not feel the effects of testosterone until month three of using it consistently. And that is so aggravating. I know, right?
Because like progesterone, you take it that day and you're like, I'm sleeping better, I'm more calm. Like, oh, I actually like, didn't wanna like slap my husband for breathing and chewing with his mouth open. So let's talk about the forms of testosterone now. So, generally speaking, I start with creams and gels.
These are often the most straightforward starting point. And the nice thing, the thing that I like about them, they're really accessible. Small dosing adjustments can be made. It can be tricky. Like when we order these gels, they come in a sachet, we're like, use a pea size amount. Um, [00:24:00] and you know, that's not gonna be completely dialed in and accurate every time you squeeze that.
And we just have to like, recognize we're doing the best we can. But the nice thing about those gels is that they are easy to titrate. So gels and creams are easy to titrate up and down. Because comparatively speaking, it's, it's not inside you like some of these other therapies, it's reversible a lot quicker because we can just stop it Now.
You're not absorbing it in your skin. So that's the pros of gels and creams and, you know, the, we can also get these compounded, but the cons are there can be variation in the compounding quality.
So I always make sure that the compounding pharmacies I'm working with, they're very transparent about how they get homogenous mixes. And I have conversations with the pharmacist, like, I wanna know any, everything about you before I work with you when it comes to absorption. That can be inconsistent for some people we see the same is true with like estrogen patches versus [00:25:00] using estrogen creams.
Um, I think the biggest con and risk of having this topical cream or gel of testosterone is the risk of transfer to others. Um, mostly children and pets. And so that is something that I will tell women if you're gonna apply it like on your inner arm and your inner thigh, like put clothes on, wash your hands, really, really good.
The other thing is that daily adherence is required. You have to apply this every single day. That can be a con for people who can't remember that, um, or who are traveling a lot. And you're like, I don't wanna travel with this open gel pack of, of testosterone. So then we might switch to like, oh, well let's do like a, you know, compounded cream.
So that travels better. Now. Another way that we can deliver testosterone is through subcutaneous injections.
Testosterone Therapy - Side: These
Dr. Brighten: are microdosed, literally microdosed compared to what we would give men. Okay. So these are not bodybuilding doses. Um, and [00:26:00] this is something that I think is just really important to understand, is that when I say microdose, I'm not saying like, oh, this is just like a tiny bit like microdosing that's like, you know, below, uh, the therapeutic effect, uh, dosing.
No, that's not what I'm saying. I'm saying it's a microdose compared to what I would give a man. Now there's no transfer risk here. That's definitely a pro. Um, we know it's gonna be absorbed, but a con is, is you get peaks, you go up and you get troughs. And so someone will be like, ah, I feel kind of agro.
Like I said, like sometimes patients are like, I feel agro, and then they're like, now I feel depressed. Like, what is happening here? So people who are sensitive, they may be really sensitive to the peaks and troughs of the injections. It's also easier to overshoot with injections and to get the side effects and side effects will take longer to reverse because this injection is gonna stay with you for a bit of time.
And so if you're like, oh, I'm already having side effects, we get to wait for your body to work that [00:27:00] out.
Now the other thing about injectables, we have to be very precise. And we have to be disciplined about the dosing. We have to make sure that we're dosing on schedule. And again, we're never overdosing. I think that is a big problem. When I say overdosing, it makes it sound like, you know, a very nefarious drug.
But, um, it just, I think it's just like such a problem that my colleagues will talk to me about. And I've had patients do it as well where they get these horrible side effects because they thought, I'm not filling it in a few days, in a few weeks, I'm just gonna do more. Now. Pellets have become really popular.
You may have heard of them. They are implanted in you, they're long acting, and there's no delay in dosing. So that's definitely a pro. Um, and you know, you don't have to think about it. You're not gonna transfer it to anyone. So there are some pros to it. I'm not a fan, however, and some people are like, well, you're biased.
And honestly, maybe I am biased, but I have just seen a lot of negative side effects with [00:28:00] pellets. So firstly, it's not reversible. That's in you. That's in you. I've had patients who have opted, they wanna go get pellets. It's your body, man, I if you choose that. Okay? They go get a pellet, they come back, they start losing hair, they start getting acne.
I'm like, okay, we gotta get you on. Like we gotta get you on some spironolactone. We gotta get you on Minoxidil. Like we gotta do something about this. There is a high risk here for Supra physiological exposure. So high doses higher than you need. And like I said, like if you are someone who's very sensitive to testosterone, the side effects can last months.
And months. And so it can be pretty miserable. And so I always think like, if you think you might wanna go the pellet route, let's try something else first with testosterone and let's just see how you feel because it's, I can, you can't adjust the pellet. It's in, it's done.
I think it's much better to see like, well, how do you do if we do a topical and we could get that dialed in and we, we can really, uh, fine tune it to you [00:29:00] and then you're like, yeah, I wanna go the pellet route because I've been tolerating this. Well, that's, that's totally your choice. But the ability to stop a pellet, like, it's just, I mean, it's just a, it's such a problem.
Uh, it's such a con for me. I just don't like things that go into you that you can't easily get out of you. Um, and that are gonna mess with your hormones. But if you used pellets and they work for you and you're like, I feel great, then I'm happy for you. Like, that's great. This is just not something I personally do.
now there are oral forms of testosterone. I never recommend those. They have far too many side effects and it's gonna go first, pass liver. It can affect your, um, your cardiovascular health, your cholesterol. So don't recommend it, but we can use a troche, something that you are just putting in your mouth and letting it dissolve there.
Um, that is still gonna have a little bit of first pass through the liver. So I don't always start with a troche. Um, I try to use the topical forms instead, but if somebody's like, look.[00:30:00]
Testoserone Therapy - Front: I
Dr. Brighten: have small kids, I have pets. Like I'm really scared of transferring it to them. They might be something that we consider.
It sometimes can be harder to maintain a steady dose. We may have some metabolic impacts. So you gotta, you gotta watch everybody for metabolic impacts when it comes to testosterone therapy. But it is an option. It does work well, and it does need to be compounded.
Testosterone Therapy - Side: So
Dr. Brighten: those are the options. And I feel like I, I was gonna do a whole segment on, uh, testosterone side effects, but I feel like I've covered them throughout the episode.
So I think what I find most important to say to you is that testosterone is very useful in women, but it's not universal and it's not neutral. It's not without side effects or consequences if done wrong and it isn't right for everyone. And so. For prescribers, they need to be responsible. They need to be careful about selecting the right person, knowing the red flags of testosterone therapy, making sure they're tracking them correctly.
This is a [00:31:00] DE, A regulated drug. So people to prescribe it need to have a DEA license. So you gotta be smart about how you're doing this. You need to use conservative dosing, start low and go slow so that you as the individual are happy. But you know, for clinicians that are listening, I know I have a lot of clinicians on the show, so your patients stay happy and we need to make sure that we continue to monitor people.
Set. You know, set your expectations up. Understand that like, I may start this and I need to track my symptoms, 'cause things usually get better over time. And then we got the full effects by three months. But you may not notice that you're feeling better. So track your symptoms and respect the entire hormone system.
If you are someone who is using testosterone therapy, for example, and you have endometriosis, you may have more aromatase activity in those lesions that may push your testosterone into estrogen. You may require more monitoring. We have to respect the entire system [00:32:00] and the individual.
Testoserone Therapy - Front: And
Dr. Brighten: remember, before considering testosterone, there are natural ways to support your own production, and sometimes those are significant.
So if you missed that episode, I wanna encourage you to go back and watch my episode on how to increase testosterone naturally in women. It's evidence-based ways to boost testosterone and helps you understand what the top causes of low testosterone are.
Testosterone Therapy - Side: And if
Dr. Brighten: you want a comprehensive framework for supporting your metabolism and your hormones through perimenopause, remember you can grab my perimenopause plan at drbrighten.com/plan D-R-B-R-I-G-H-T-E-N.com/plan. And as always, thank you for listening to the Dr. Brighten Show. It is always a pleasure to share this time with you.
Please leave me a comment, consider subscribing and let me know what else you'd like to hear on the show.